Predictors of mortality and poor outcome in cancer patients with E. faecium bloodstream infection
Predictores de mortalidad y mal pronóstico en el paciente oncológico con bacteriemia enterocócica
A. Pérez-García1, J.J. Beunza2, A. Gea2, M.F. Landecho3, E. Mauleón3, J.L. del Pozo4
1. Departament of Clinical Microbiology. Clínica Universidad de Navarra. Pamplona. Spain.
2. Departament of Preventive Medicine and Public Health. Universidad de Navarra. Pamplona. Spain.
3. Departament of Internal Medicine. Clínica Universidad de Navarra. Pamplona. Spain. ]]>
4. Division of Infectous Diseases and Clinical Microbiology. Clínica Universidad de Navarra Pamplona. Spain.
ABSTRACT
Background. To analyze predictors of mortality and poor outcome in cancer patients diagnosed with E. faecium bloodstream infection.
Methods. Demographic, clinical and microbiological data were collected (January 1998-June 2011).
Results. After multivariate analysis, presence of a urinary catheter was associated with a worse 7-day prognosis, and higher mortality at discharge. A high Charlson index was also associated with higher 7-day mortality.
Conclusion. Presence of a urinary catheter was associated with poor 7-day prognosis and higher mortality at discharge in the present series.
Key words: Bloodstream infection. Enterococcus faecium. Cancer. Predictors.
Fundamento. Analizar los predictores de mortalidad y mal pronóstico en el paciente oncológico diagnosticado de bacteriemia por E. faecium.
Métodos. Se analizaron datos demográficos, clínicos y microbiológicos (Enero 1998-Junio 2011).
Resultados. El análisis multivariable demostró que la presencia de una sonda urinaria se asoció a mal pronóstico a los 7 días y alta mortalidad del paciente al final del estudio. Un índice de Charlson elevado se asoció a un aumento en la mortalidad a los 7 días.
Conclusión. En nuestro estudio, la presencia de sonda urinaria se asoció con mal pronóstico del paciente a los 7 días y aumento de la mortalidad.
Palabras clave: Bacteriemia. Enterococcus faecium. Cáncer. Predictores.
Introduction
Enterococcus spp. is an important cause of serious infections such as bloodstream infection and endocarditis1,2. In the United States, Enterococcus spp. is the second most common cause of nosocomial bloodstream infection (BSI), representing 25% of all isolates3. Enterococcus spp. represents 10% of all blood cultures isolates in Europe and their incidence is rising4,5. This is in part because it often occurs in patients with prolonged hospitalization, co-morbidities, or who are undergoing instrumental manipulation or are under antibiotic pressure4-6. Enterococci, compared to other Gram-positive cocci such as S. aureus or S. pyogenes, has low pathogenicity and lacks important virulence factors. Despite that, it is able to form biofilms associated with biomedical devices. Enterococcus spp is inherently resistant to certain antibiotics used frequently, but also has an innate ability to acquire new mechanisms of resistance especially in the case of E. faecium5. Despite E. faecalis is the specie most frequently isolated from cultures, E. faecium has been described as a microorganism with more clinical relevance than E. faecalis (because of its virulence and main resistant mechanisms). In addition, in the case of BSI secondary, the E. faecium isolation frequency is greater than E.faecalis7,8. Enterococcal bloodstream infection has a specific mortality, even with adequate treatment, of 31-37% depending on the series9,10. The present study was conducted to analyze predictors of mortality and outcome in cancer patients diagnosed with Enterococcus faecium BSI.
]]> Patients and methods
Longitudinal retrospective study (January 1998-June 2011) of consecutive patients diagnosed with Enterococcus spp. BSI in our center, Clínica Universidad de Navarra, Spain. We collected demographic, clinical, microbiological, antibiotic exposure, treatment and prognosis of individual patients included in the study. Outcomes were defined in three different times (72 hours, 7 days, and at discharge). It was estimated the median length of stay of each patient as a consequence of the BSI episode, keeping in mind that day 0 consisted of blood culture extraction. Blood cultures studied for each patient were processed in the microbiology laboratory. Identification of the isolates and susceptibility testing were performed using standard bacteriological methods and an automated system (Vitek II® System, bioMerieux, Durham, NC, USA) in accordance with the CLSI® guidelines (CLSI Performance Standards for Susceptibility Testing).
Data was collected from each patient by a previously designed form. Epidemiological data included the following: sex, age, hospitalization ward (medical wards, surgical wards or ICUs), previous episodes of hospitalization, antibiotic use, surgery, or ICU admissions, means of acquisition (community, healthcare-associated or hospital acquired), exogenous risk factor for acquiring the BSI, underlying diseases and their severity (Charlson index of co-morbidity score)11,12. Microbiological data included the following: mono- or polymicrobial etiology, enterococcal species isolated (E. faecalis or E. faecium), vancomycin MIC (µg/mL), ampicillin MIC (µg/mL) and gentamicin synergy (detection of high-level resistance to aminoglycosides). Clinical data included the following: source of the BSI, antimicrobial therapy and duration of treatment. Also collected as a variable of study if the patient had developed sepsis (sepsis, severe sepsis or septic shock) as a result of BSI13. Outcomes were defined as either "clinical cure" (decrease of temperature or ausence of fever, 50% decrease of infection parameters with reference to the levels corresponding to day 0 and/ or negative hemocultive) or "not clinical cure" at three different times: 72 hours, 7 days, and at discharge. Finally, we calculated the total crude mortality and mortality attributable to bloodstream infection. Death was attributable to E. faecium BSI if at least one of the following was present: i) positive blood culture at the time of death; ii) persistent signs and symptoms of infection due to that microorganism at death; iii) death within the first week after the isolation of the microorganism in blood culture.
We studied the relationship among all these variables with respect to every outcome we had defined. Logistic regression was used for uni- and multivariate analysis of associations with every outcome. Results with a P value <0.05 were considered to be statistically significant. All computations were performed with SPSS-Software (version 15.00; SPSS, INC., Chicago, IL).
Results
Included in the study were 122 consecutive patients who had episodes of clinically significant enterococcal BSI. Seventy out of 122 (57,4%) were diagnosed with malignancy (solid tumors and haematological tumors). Of these seventy patients, E. faecium was isolated from 34 blood cultures in 28 patients.
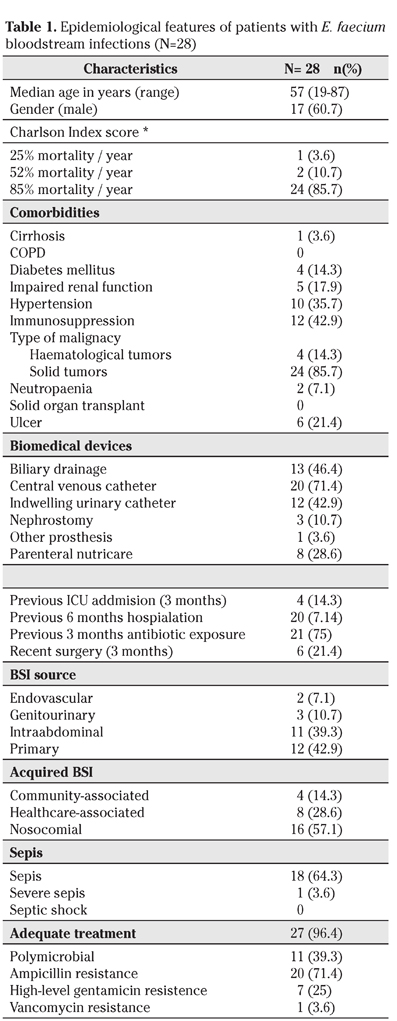
The initial clinical and demographic characteristics of the patients are shown in table 1. Most of the patients (81%) had some type of medical device at the time of BSI [i.e, central vascular catheter (71%), indwelling urinary catheter (43%)]. Twenty out of 28 patients (71%) had been hospitalized in the 6 months prior to BSI, with 14% admitted to ICU; 75% had received antimicrobial therapy in the 3 months prior to BSI. Sixteen patients (57%) were diagnosed with a hospital-acquired BSI. None of the cases were associated with clustering or outbreak during the study period. BSI source could not be determined in 12 episodes (43%). Polymicrobial episodes were more likely to be hospital-acquired (9 cases out of 11). Related deaths were higher in monomicrobial bloodstream infection than in polymicrobial (five versus zero episodes). Sepsis and septic shock were present at BSI diagnosis in 19 patients (67%) and 4 (14%) patients had to be admitted at the ICU because of the infection. Relapse of BSI was documented in six (21%) patients. Four of these patients presented a poor outcome at 72 hours and 7 days. Only one patient received inappropriate initial antimicrobial therapy. Glycopeptides were the most frequent previously administered antibiotics (54%), followed by aminoglycosides (36%) and quinolones (21%). The median length of stay was 29 days (SD: 30 days) for all patients. Total and specific BSI mortality, at discharge, were 36% and 18%, respectively (Table 2). Multivariate logistic regression analysis showed that presence of an indwelling urinary catheter was associated with a worse 7-days outcome (OR, 26.92; 95% CI, 2.28-317; P= 0.009), and a higher mortality at discharge (OR, 9.14; 95% CI, 1.10-75.8; P= 0.040). A high Charlson index score was found to be an independent predictor (OR, 2.17; CI, 0.93-5.07; P= 0.071) for 7-days mortality (Table 3).


Discussion
The presence of a foreign body is considered to be a potential extrinsic risk factor as well as another potential way of acquiring infection or development of resistances to antimicrobial agents6. In our study, up to 71% of all patients had a central intravenous catheter and 43% carried an indwelling urinary catheter at the BSI moment. However, while the presence of this last one (indwelling urinary catheter) has been demonstrated by the analysis as having statistical differences [worse 7-days outcome (OR, 26.92; 95% CI, 2.28-317; p= 0.009), and mortality at discharge (OR, 9.14; 95% CI, 1.10-75.8; P= 0.040)], that does not happen with the central venous catheter (no significative differences). Caballero-Granado et al, in his study about the attibutable mortality rate and duration hospital stay related to the enterococcal BSI, showed that the presence of an indwelling urinary catheter was associated with global mortality increase14. In their study, Patterson et al., defined the presence of an indwelling urinary catheter as a potential risk factor for the Enterococcus spp. high-level gentamycin acquiring resistance15. Similar to this, Fortún et al, in their study, demonstrated that the presence of an indwelling urinary catheter not only was a predictor of ampicillin resistance acquired but it also was associated to higher patient´s mortality16. There are several studies about the etiologic and risk factors in nosocomial infections. One of them is the Akkoyun´s study which, in addition to analyzing these etiologic causes or risk factors, the author exposed that 37.8% of all the indwelling urinary catheterization episodes were unnecessary17. Another possible explanation may be that, despite the relevance of E. faecium as a cause of BSI, it is not a common microorganism involved in the origin of intravascular catheter infection; hence, the low numbers of BSI with endovascular source in our study and its better prognosis. Our study had some limitations, including the retrospective nature of the study, the limited number of cases, the absence of a significant number of vancomycin-resistance isolates, the long period of study and therapeutic developments in this disease. However, we have carried a thorough analysis of all the potential variables that could influence the outcome of these patients.
Similar to other studies that have been described4,5, enterococcal bloodstream infection is related to patients with a high number of co-morbidities and severe underlying illnesses. In our study, 96% of all patients presented a Charlson index higher than 2. Patient´s comorbidities are not the only unique risk factors. Along with the features of our population, we could observe in our study how a high number of patients presented a previous antibiotic exposure (75%) and previous hospitalization (71.4%). These variables along with the previous ICU admission are considered by a number of studies as potential risk factor to the infection acquired and to the development of resistances to antimicrobial agents. In Furuno´s study, the previous antibiotic exposure and previous hospitalization are risk factors for the E. faecalis and the E. faecium acquired18. In the same way, in Patterson´s and Caballero´s studies postulated that the previous use of antibiotics was related to fatal outcome14,15. We observed that 57% of the BSI episodes were hospital-acquired. This concurs with that published by other studies in which the majority of the episodes enterococcal BSI episodes are hospital acquired5,6. A 39% of the episodes were polymicrobial. We already know, as demonstrated in Patterson et al study, that the polymicrobial enterococcal BSI have better prognosis and outcome than monomicrobial15.
Several studies talk about the importance of choosing the appropriate empirical treatment19. These studies have demonstrated that correct selection and early initiation of treatment is associated with lower attributable mortality and therefore better patient prognosis. Caballero-Granado et al. demonstrated that inappropriate treatment was a poor prognostic factor14. In our series, 96% of our patients received adequate treatment. Vancomycin, in combination with other antibiotics, was the drug most used in the BSI´s treatment.
In our series severity of illness and the presence of an indwelling urinary catheter proved to be strong prognostic predictors of mortality in cancer patients with E. faecium BSI. A good strategy to create the safest patient situation would be to avoid unnecessary catheter use and, when necessary use them for the shortest period of time. Proper use of an indwelling urinary catheter and other biomedical devices can reduce morbidity and mortality associated with bloodstream infection and improve patients outcomes.
]]>References
1. Martínez-Marcos FJ, Lomas-Cabezas JM, Hidalgo-Tenorio C, de la Torre-Lima J, Plata-Ciezar A, Reguera-Iglesias JM, et al. Grupo para el Estudio de las Infecciones Cardiovasculares de la Sociedad Andaluza de Enfermedades Infecciosas. Endocarditis por enterococo: análisis multicéntrico de 76 casos. Enferm Infecc Microbiol Clin 2009; 27: 571-579. [ Links ]
2. Sava IG, Heikens E, Huebner J. Pathogenesis and immunity in enterococcal infections. Clin Microbiol Infect 2010; 16: 533-540. [ Links ]
3. McKinnell JA, Patel M, Shirley RM, Kunz DF, Moser SA, Baddley JW. Observational study of the epidemiology and outcomes of vancomycin-resistant enterococcus bacteraemia treated with newer antimicrobial agents. Epidemiol Infect 2011; 139: 1342-1350. [ Links ]
4. Conde-Estévez D, Grau S, Albanell J, Terradas R, Salvado M, Knobel H. Clinical characteristics and outcomes of patients with vancomycin-susceptible Enterococcus faecalis and Enterococcus faecium bacteraemia in cancer patients. Eur J Clin Microbiol Infect Dis 2011; 30: 103-108. [ Links ]
]]>5. Martínez-Odriozola P, Muñoz-Sánchez J, Gutiérrez-Macías A, Arriola-Martínez P, Montero-Aparicio E, Ezpeleta-Baquedano C, et al. Análisis de 182 episodios de bacteriemia por enterococo: Estudio de la epidemiología, microbiología, y evolución clínica. Enferm Infecc Microbiol Clin 2007; 25: 503-507. [ Links ]
6. McBride SJ, Upton A, Roberts SA. Clinical characteristics and outcomes of patients with vancomycin-susceptible Enterococcus faecalis and Enterococcus faecium bacteraemia-a five-year retrospective review. Eur J Clin Microbiol Infect Dis 2010; 29: 107-114. [ Links ]
7. Cantón R, Ruiz-Garbajosa P. Infecciones causadas por bacterias grampositivas multirresistentes (Staphylococcus aureus y Enterococcus spp.). Enferm Infecc Microbiol Clin 2013; 31: 543-551. [ Links ]
8. ENVIN-HELICS. Estudio Nacional de vigilancia de infección nosocomial en Servicio de Medicina Intensiva. Sociedad Española de Medicina Intensiva Crítica y Unidades Coronarias (SEMICYUC) Grupo de trabajo de Enfermedades Infecciosas. 2011; http://hws.vhebron.net/envin-helics/Help/Informe ENVIN-UCI 2011.pdf. [ Links ]
9. Landry SL, Kaiser DL, Wenzel RP. Hospital stay and mortality attributed to nosocomial enterococcal bacteremia: a controlled study. Am J Infect Control 1989; 17: 323-329. [ Links ]
]]>10. Lautenbach E, Bilker WB, Brennan PJ. Enterococcal bacteremia: risk factors for vancomycin resistance and predictors of mortality. Infect Control Hosp Epidemiol 1999; 20: 318-323. [ Links ]
11. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis 1987; 40: 373-383. [ Links ]
12. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol 1994; 47: 1245-1251. [ Links ]
13. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med 2003; 29: 530-538. [ Links ]
14. Caballero-Granado FJ, Becerril B, Cuberos L, Bernabeu M, Cisneros JM, Pachón J. Attributable mortality rate and duration of hospital stay associated with enterococcal bacteremia. Clin Infect Dis 2001; 32: 587-594. [ Links ]
]]>15. Patterson JE, Sweeney AH, Simms M, Carley N, Mangi R, Sabetta J, et al. An analysis of 110 serious enterococcal infections. epidemiology, antibiotic susceptibility, and outcome. Medicine (Baltimore) 1995; 74: 191-200. [ Links ]
16. Fortún J, Coque TM, Martín-Dávila P, Moreno L, Cantón R, Loza E, et al. Risk factors associated with ampicillin resistance in patients with bacteraemia caused by Enterococcus faecium. J Antimicrob Chemother 2002; 50: 1003-1009. [ Links ]
17. Akkoyun S, Kuloglu F, Tokuc B. Etiologic agents and risk factors in nosocomial urinary tract infections. (Article in Turkish). Mikrobiyol Bul 2008; 42: 245-254. [ Links ]
18. Furuno JP, Harris AD, Wright MO, McGregor JC, Venezia RA, Zhu J, et al. Prediction rules to identify patients with methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci upon hospital admission. Am J Infect Control 2004; 32: 436-440. [ Links ]
19. Nazar JR, Lavados A, Daher O, Bischoff MC. Análisis microbiológico y epidemiológico, y evolución clínica de los pacientes con bacteriemia en el Hospital de Zona de Esquel en el periodo 2007-2009. Rev Argent Microbiol 2010; 42: 151-164. [ Links ]
]]>
![]() Correspondence:
Correspondence:
Alejandra Pérez García
Departament of Clinical Microbiology
Clínica Universitaria de Navarra
Avda. Pío XII, 36
31008 Pamplona. Navarra
Recepción: 17 de septiembre de 2014
Aceptación provisional: 11 de diciembre de 2014 ]]>
Aceptación definitiva: 20 de enero de 2015