Progressive hemifacial atrophy Case report
Thiago Pastor da Silva Pinheiro 1, Camila Camarinha da Silva 2, Carolina Souza Limeira da Silveira 2,
Patrícia Cristina Ereno Botelho 3, Maria das Graças Rodrigues Pinheiro 4, João de Jesus Viana Pinheiro 5
(1) DDS, Department of Estomatology, School of Dentistry, University Center of Pará
(2) Student of Department of Oral Pathology, School of Dentistry of Federal University of Pará
(3) DDS, Orthodontist ]]>
(4) MS, Department of Estomatology, School of Dentistry, University Center of Pará
(5) PhD, Universitary Hospital João de Barros Barreto, Department of Oral Pathology,
School of Dentistry of Federal University of Pará
ABSTRACT
Progressive Hemifacial Atrophy, also known as Parry-Romberg Syndrome, is an uncommon degenerative and poorly understood condition. It is characterized by a slow and progressive atrophy affecting one side of the face. The incidence and the cause of this alteration is unknown. A cerebral disturbance of fat metabolism has been proposed as a primary cause. This can be the result of a trophic malformation of Cervical Sympathetic Nervous System. Possible factors that are involved in the pathogenesis include trauma, viral infections, heredity, endocrine disturbances and auto-immunity, among others. The most common complications that appear in association to this health disorder are: trigeminal neuritis, facial paresthesia, severe headache and epilepsy, being this last one the most frequent complication of the Central Nervous System. Characteristically, the atrophy progresses slowly for several years and, soon after, it become stable. Now, plastic surgery with graft of autogenous fat can be performed, after stabilization of the disease, to correct the deformity. Orthodontic treatment can help in the correction of any associated malformation. The objective of this work is, through the presentation of a clinical case, to accomplish a literature review concerning general characteristics, etiology, physiopathology, differential diagnosis and treatment of progressive hemifacial atrophy.
Key words: Hemifacial atrophy, Parry-Romberg syndrome, physiopathology, treatment.
]]> Introduction
Progressive Hemifacial Atrophy, also known as Parry-Romberg Syndrome, is an uncommon degenerative condition characterized by a slow and progressive atrophy, generally unilateral, of facial tissues, including muscles, bones and skin (1, 2). More than an aesthetic trouble, this illness bring several functional and psychological problems, when a "symmetric" face lose its identity. The incidence and cause of this alteration is unknown. A cerebral disturbance on fat metabolism has been proposed as a primary cause (3, 4). Trauma, viral infections, endocrine disturbances, auto-immunity and heredity are believed to be associated to the pathogenesis of the disease (5-9).
Frequently, the onset of this syndrome occur along first and second decades of life. Characteristically, the atrophy progress slowly during many years and, then, it become stable (5, 10-12). Alterations concerning involvement, duration and deformity can stabilize in any stage of growing and development (2, 5). Patients who manifest atrophy in early ages, have bigger repercussions (11).
This syndrome seems to have higher incidence in women (1, 3, 7). The extension of the atrophy is frequently limited to on one side of the face, and the ipsilateral involvement of body is rare (2). 5% to 10% of cases were described as being bilateral (6).
The most important features of this pathology are the enophthalmy, the deviation of mouth and nose to the affected side, and unilateral exposition of teeth (when lips are involved) (7), among others.
Parry-Romberg Syndrome is an auto-limitable condition and there is no cure. Affected patients should have multidisciplinary attendance of physicians, dentists, phonoaudiologists and psychologists. Treatment were developed trying to give a better appearance to carriers of this syndrome. Nowadays, cosmetic surgeries with autogenous fat graft, injections of silicone or bovine collagen, and inorganic implants are some alternatives to correct deformities (13). Besides esthetic improvement, symptomatic treatment for neurological disorders is indicated (9).
The objective of this work is, through the presentation of a clinical case, to accomplish a literature review concerning general characteristics, etiology, physiopathology, differential diagnosis and treatment of progressive hemifacial atrophy.
Case Report
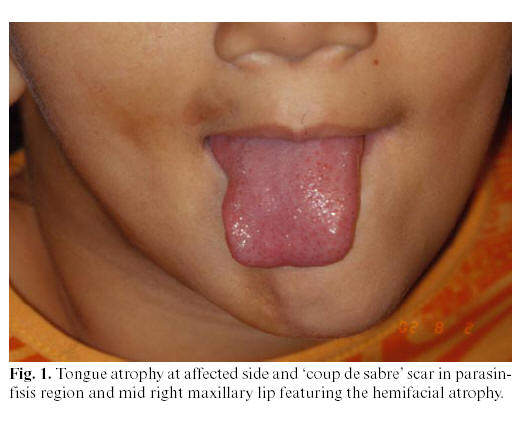
In 2001, an 8-year-old female patient, resident in Belém, State of Pará, Brazil, was conducted do the radiological clinic for orthodontic documentation. During the physical examination, it was noted that this patient presented facial asymmetry with a marked hypoplasia of the right side of the face, with deviation of lips and nose, with a big linear dark scar (coup de sabre) in the right side of mandibular mentum region, enophthalmy in right eye region and areas of hyperpigmentation on the affected skin. Intraorally, the most relevant alteration was the unilateral atrophy of tongue (Figure 1). Radiographically, it was observed an atrophic root development or a pathologic reabsorption of permanent teeth numbers 34, 33, 41, 42, 43, 44, 45, 46 and 47 (Figure 2).
]]> 
The patient presented good health condition, without any sickness that would explain the cause of that facial asymmetry. Photos of previous years were requested to the responsible for the patient, who provided them from the 1st until the 8th year of age. Clinical signs of the disturb were just noticed from the 6th year onwards (Figure 3 A, B, C).

With these clinical and radiologic findings, the diagnosis was of progressive hemifacial atrophy. At present, the patient is being periodically reviewed until atrophic manifestation stops and specific intervention could be accomplished.
In 2003, at age of 10, a new photographic and radiographic documentation was done in order to analyze the evolution of the case. Extraorally, there was an aggravation of clinical signs observed two years ago, such as enophthalmy, hypoplasia of right hemiface, with deviation of lips and nose, and also cutaneous hyperpigmentation. During an intraoral exam, it was observed the persistence of the canine and the first molar deciduous teeth, as well as dental crowding. Radiographically, it was noticed an image suggestive of pathologic root reabsorption of teeth number 14, 15, 16, 17, 41, 42, 43, 44, 45, 46 and 47, as well as impactation of element 45 by 84 and of element 47 by 48 (developing tooth).
Discussion
Progressive hemifacial atrophy, as described in the case above, is a rare pathology, of unknown cause, whose degenerative condition affect not only the esthetic, but also the functionality of the attained hemiface.
]]> Clinically, the skin can be dry and with a dark pigmentation. Some patients present a demarcation line between normal and abnormal skin, reminding a big linear scar, known as coup de sabre, as we could notice in the case reported. Ocular involvement is common, and the most frequent manifestation is the enophthalmy, due to fat loss around the orbit, as was observed in our patient. The eye usually works normally. Even not noticed in the present case, the ear can be smaller than normal ones due to the atrophy (5). There may be localized areas of alopecia. Occasionally, there may be some neurological complications, such as trigeminal neuralgia, facial paresthesia, severe headache and contralateral epilepsy (1, 11, 14-16), this last being the most common complication (17). Mouth and nose are deviated to the affected side, deviating also facial and dental midlines. Atrophy of superior lip led the anterior teeth to be exposed, and there may be also unilateral atrophy of tongue. Our case showed clearly those features of facial asymmetry and tongue atrophy. Radiographically, teeth of affected side can present some deficiency in root development and, consequently, delayed eruption. However, the affected teeth are normal and vital clinically. This situation occurred with our patient, as most of her teeth of the affected side presented a reabsorption/malformation of their roots, causing delayed eruption and dental crowding. Very often, there is unilateral posterior crossbite, as a result of jaw hypoplasia and delayed teeth eruption (4, 10). The intraoral soft tissue and chewing muscles are, sometimes, normal, without any movement, speeching or deglutition implications (5, 7). Histologically, atrophy of epidermis, dermis and subcutaneous tissue are observed (7). Variable infiltrate of lymphocytes and monocytes at dermis (11, 7) and lack of subcutaneous fat in the affected tissue are also characteristic (7). Besides, it can be identified degenerative alterations on vascular endothelia in electron microscopy (7).The treatment is usually based on reposition of adipose tissue that was lost due to atrophy (12). Autogenous fat grafts, cartilage grafts, silicon injections and prostheses, bovine collagen and inorganic implants are some alternatives to esthetic correction of the atrophy (12, 13). However, these treatment modalities resolve just momentarily the good appearance, whereas all the structure projected in the cosmetic surgery is lost with time, due to gravity action, and the patient needs a new intervention. Moreover, a backing treatment is indicated to functional and neurological troubles. The cosmetic treatment is just recommended when the illness stops its evolution, so this is the reason why our patient hasnt been submitted to any surgical intervention yet.
Precocious diagnostic is relevant, mainly in cases of systemic sicknesses with idiopathic origin, in which a simple anamnesis and a conventional clinical exam do not give enough data for a precise diagnosis and a suitable treatment.
References
1. Jurkiewicz MJ, Nahai F. The use of free revascularized grafts in the amelioration of hemifacial atrophy. Plast Reconstr Surg 1985;76:44-55. [ Links ]
2. Lakhani PK, David TJ. Progressive hemifacial atrophy with scleroderma and ipsilateral limb wasting (Parry Romberg Syndrome). J R Soc Med 1984;77:138-9. [ Links ]
3. Finesilver B, Rosow HN. Total hemiatrophy. JAMA 1938;5:366-8. [ Links ]
4. Foster TD. The effects of hemifacial atrophy of dental growth. Br Dent J 1979;146:148-50. [ Links ]
5. Mazzeo N, Fisher JG, Mayer MH, Mathieu GP, Mcade FGG. Progressive hemifacial atrophy (Parry Romberg Syndrome). Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:30-5. [ Links ]
6. Miller MT, Sloane H, Goldberg MF, Grisolano J, Frenkel M, Mafee MF. Progressive hemifacial atrophy (Parry Romberg Disease). J Pediatr Oftamol Strabismus 1987;24:27-36. [ Links ]
7. Pensler JM, Murphy GF, Muliken JB. Clinical and ultra-structural studies of Romberg´s hemifacial atrophy. Plast Reconstr Surg 1990;85:669-76. [ Links ]
8. Shaffer WG, Hine MK, Levy BM, eds. Textbook of oral pathology. Philadelphia: WB Saunders; 1983. p. 9-10. [ Links ]
9. Zafarulla MY. Progressive hemifacial atrophy: a case report. Br J Ophthalmol 1985;69:545-7. [ Links ]
10. Moore MH, Wong KS, Proudman TW, David DJ. Progressive hemifacial atrophy (Romberg´s Disease): skeletal involvement and treatment. Br J Plast Surg 1993; 46: 39-44. [ Links ]
11. Neville BW, Damm DD, Allen CN, Bouquout JE, eds. Patologia oral e Maxilofacial. Rio de Janeiro: Guanabara Koogan; 1998. p. 35. [ Links ]
12. Roddi R, Riggio E, Gilbert PM, Houvius SER, Vaandrager JM, van der Meulen JCH. Clinical evaluation of techiniques used in the surgical treatment of progressive hemifacial atrophy. J Craniomaxilofac Surg 1994;22:23-32. [ Links ]
13. de la Fuente A, Jimenez A. Latissimus dorsi free flap for restauration of facial contour defects. Ann Plast Surg 1989;22:1-8. [ Links ]
14. Gorlin RJ, Pinborg JJ, eds. Syndromes of the head and neck. New York: McGraw Hill; 1964. p. 475 7. [ Links ]
15. Roed-Petersen B. Hemifacial lipodystrophy report of a case. Oral Surg Oral Med Oral Pathol 1979;43:230-2. [ Links ]
16. Sagild JC, Alving J. Hemiplegic migraine and progressive hemifacial atrophy. Ann Neurol 1985;17:620. [ Links ]
17. Chbicheb M, Gelot A, Rivier F, Roubertie A, Humbert Claude V, Coubes P. et al. Parry-Romberg´s syndrome and epilepsy. Rev Neurol 2005;161:92-7. [ Links ]
![]() Correspondence
Correspondence
Dr. João de Jesus Viana Pinheiro
Av. Almirante Wandenkolk, 1243,1006
Umarizal. Belém-Pará-Brazil
ZIP Code: 66050-030
E-mail- radface@hotmail.com