Angiomyolipoma of the upper lip: case report and review of the literature
Andréia Aparecida da Silva1, Roman Carlos2, Elisa Contreras2, Oslei Paes de Almeida3, Márcio Ajudarte Lopes3, Pablo Agustín Vargas3
(1) PhD student. Department of Oral Diagnosis, Oral Pathology Division, Dental School of Piracicaba, State University of Campinas, Piracicaba, Brazil
(2) DDS. Guatemala Centre of Oral Medicine, Mariano Galvez University, Guatemala
(3) DDS, PhD. Department of Oral Diagnosis, Oral Pathology Division, Dental School of Piracicaba, State University of Campinas, Piracicaba, Brazil
ABSTRACT
Angiomyolipoma (AML) is a hamartomatous growth that usually affects the kidney. One third of patients with AML present with manifestations of tuberous sclerosis. Oral AML is rare with only 6 cases reported in the English-language literature. In the present case, AML was located in the upper lip of a 43 year-old woman. Clinically, it presented as a firm nodule, well circumscribed and measuring 1x2 cm. It was surgically excised. Histopathological analysis showed a lesion composed of an admixture of smooth muscle cells, blood vessels, and adipose tissue. The immunohistochemical study revealed positivity for vimentin, smooth muscle actin, pan specific muscle actin and desmin. CD68, CD34 and mast cell antibodies showed focal immunoreactivity. S100 protein, Ki-67, and HMB-45 were negative. Based on these histological and immunohistochemical features the diagnosis was of oral AML. No recurrence was observed after 2 years of follow-up.
Key words: Oral angiomyolipoma, immunohistochemistry, tuberous sclerosis, upper lip.
RESUMEN
El angiomiolipoma (AML) es un crecimiento tumoral hamartomatoso que usualmente afecta el riñón. Un tercio de los pacientes con AML cursan con manifestaciones de esclerosis tuberosa. El AML de la cavidad oral es raro y hasta la fecha se han reportado 6 casos en la literatura de habla inglesa. El presente caso constituye un AML localizado en el labio superior en una paciente de 43 años de edad. Clínicamente era un nódulo de 1x2cm., firme y bien circunscrito. Fue removido quirúrgicamente. El estudio histológico reveló una lesión compuesta por una mezcla de músculo liso, vasos sanguíneos y tejido adiposo. El análisis inmunohistoquímico reveló positividad para vimentina, actina alfa de músculo liso, pan-actina músculo específico y desmina. CD68, CD34 y anticuerpos anti-mastocitos mostraron inmunoreactividad focal. Proteína S-100, Ki-67 y HMB-45 fueron negativos. Basados en estas características histológicas e inmunohistoquímicas se estableció el diagnóstico de AML oral. No se ha observado recurrencia 2 años después de su remoción.
Palabras clave: Angiomiolipoma oral, esclerosis tuberosa, inmunohistoquimica, labio superior.
Introduction
]]> Angiomyolipoma (AML) is a tumour that commonly affects the kidney (1), and one third of patients present symptoms of tuberous sclerosis (TS). Extrarenal AML is uncommon and it is usually not associated with TS (2). Among the extrarenal sites, the liver is the most frequently involved, however, some cases have been reported in other sites such as the mediastinum, abdominal wall, heart, spermatic cord, vaginal wall, fallopian tube, oral cavity, oropharynx, nasal cavity, lung, spinal cord, penis, retroperitonium, salivary gland and skin (1-6). According to the English-language literature, only 6 cases of oral AML have been reported.The histological diagnosis is based on the triad: mature adipose tissue, convoluted thick-walled blood vessels and irregularly arranged sheets, and interlacing fascicles of smooth muscle (4). Extrarenal AML, despite the histological similarities, differs in several ways from renal AML. AML of the kidney is composed of smooth muscle cells, blood vessels and mature fat cell, with a variable proportion of each component in individual tumours (1,5), but they can be invasive and may recur. Extrarenal AML is usually well circumscribed, easily resected, and HMB-45 (melanocyte marker) negative. However, renal AML associated with TS is positive for HMB-45. The purpose of the present report is to describe the first case of oral AML located in the upper lip, and discuss its histological and immunohistochemical features.
Case Report
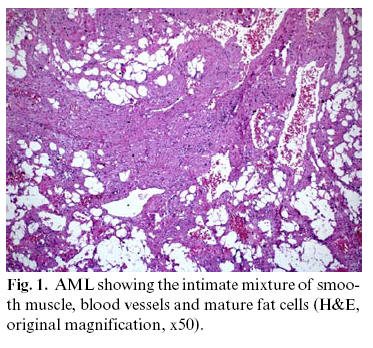
A 43-year-old Guatemalan woman was referred to the dental clinic for evaluation of a painful mass on the upper lip, crossing the midline. According to the patient the lesion had been present for 6 years. On palpation, it was of firm consistency, well circumscribed with overlying normal appearing mucosa. It measured 2 cm at its greatest dimension. The medical history was unremarkable. Under local anesthesia, the lesion was easily resected. Microscopically, it showed a well-demarcated lesion surrounded by an incomplete capsule. The tissue was composed of an admixture of smooth muscle cell, blood vessels, and adipose tissue (Fig.1). Smooth muscle cells were of different sizes and arranged around vascular spaces, with the vessel walls showing foci of hyalinization. The following antibodies were applied in order to diagnose our case: Alpha smooth muscle actin (clone 1A4, dilution 1: 400, Dako A/S, Glostrup, Denmark), Pan specific muscle actin (clone HHF-35, dilution 1:800, Dako A/S, Glostrup, Denmark), Vimentin (clone Vim 3B4, dilution 1: 400, Dako A/S, Glostrup, Denmark), Desmin (clone D33, dilution 1:1000, Dako A/S, Glostrup, Denmark), CD34 (clone QBEnd10, dilution 1:50, Dako A/S, Glostrup, Denmark), Ki-67 (clone Ki-S5, dilution 1:200, Dako A/S, Glostrup, Denmark), S-100 protein (dilution 1: 10000, Dako A/S, Glostrup, Denmark), CD68 (clone PGM1, dilution 1:400, Dako A/S, Glostrup, Denmark), Mast cell antibody (clone AA1, dilution 1: 10000, Dako A/S, Glostrup, Denmark) and HMB-45 (dilution 1:200, Dako A/S, Glostrup, Denmark).
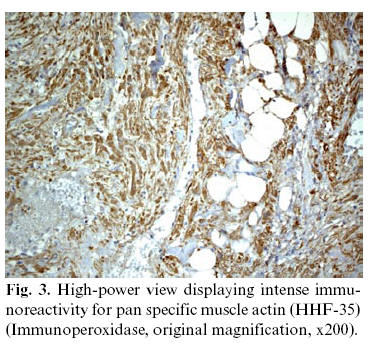
For the immunohistochemical reaction we used citrate buffer pH 6,0 for antigen recuperation and 3% hydrogen peroxidase for endogen peroxidase inactivation. For detection of the primary antibodies, we used secondary antibody conjugated with streptavidin-biotin-peroxidase (Strep ABComplex/HRP Duet, Mouse/Rabbit, Dako A/S, Glostrup, Denmark), which were revealed using diaminobenzidine and counterstained with hematoxylin of Carazzi. The immunoexpression was considered positive or negative. Immunohistochemical findings showed intense immunoreactivity for vimentin, alpha smooth muscle actin, pan muscle actin and desmin (Figs. 2-3-4). CD68, CD34 and mast cell antibodies showed focal positivity. S100 protein, Ki-67 and HMB-45 were negative. Based on these findings the diagnosis of oral AML was confirmed. Renal ultrasonography was normal and the patient had no family history of TS. After 2 years of follow-up, no recurrence has been observed.


Discussion
Stout (1953) (7) proposed the term benign mesenchymoma to indicate a benign lesion composed of two or more mesenchymal tissue components. Accordingly, AML could be considered a type of benign mesenchymoma.
As discussed by Shimizu et al (8) and Val Bernal and Mira (1996) (9), the term angiomyolipoma is preferred for this entity since it provides more information regarding the morphological nature of the lesion (2).
TS is a hereditary syndrome transmissible through genetic mutation involving chromosomes 9 or 16, but it is also recognized in a sporadic form that probably occurs due to spontaneous mutation. Patients exhibit angiofibromatosis, epilepsy or mental retardation, cutaneous lesions such as hypomelanotic spots and angiofibromas ("adenoma sebaceum"). TS is associated with intracranial and extracranial tumours, among which renal AMLs. In contrast, this association has been rarely reported in extrarenal AML (2). The current case did not present intra or extraoral findings of the TS and the renal ultrasonography was normal.
Six cases of oral AML have been previously reported in the English-language literature (Table 1). However, one of these cases, reported by Ide et al (4) lacked the classic features of oral AML, according to these authors, who suggested the term angiomyolipomatous hamartoma. In our opinion, the lesion contained the 3 types of mesenchymal tissues that confirmed AML, so we decided to classify it as AML in accordance with the reported findings.
Oral sites affected by AML included the hard palate (1,3,10), lower lip (10), lateral border of the tongue (4) and buccal mucosa (11). These lesions affected adults between the fourth and sixth decade of life and showed predilection for women. The mean size of the tumour was 1,0 cm (0,6 cm 2 cm). The mean duration of the oral AML was of 8.3 years (10 months 14 years). These clinical features are similar to our case, except for the location, being the first case described affecting the upper lip. Recently, López et al. (11) reported one case of oral AML associated with TS, which affected the lower lip and buccal mucosa. According to these authors oral AML associated with TS seems also to be a single presentation.
Renal AML is a distinctive tumour composed of smooth muscle cells, vessels and mature fat cells, with the proportion of each component varying in individual tumours (5). Liver and renal AMLs typically show epithelioid cells, which are positive for anti-HMB 45 antibody in many cases, but HMB-45 positivity can be weaker or absent in spindle cells (2). The present case was positive for vimentin, alpha smooth muscle actin, pan muscle actin and desmin, which are usually expressed in mesenchymal tumors with muscle differentiation. It was negative for S-100 protein, and showed some cells with epithelioid appearance; however they were negative for HMB-45. Our results agree with the positivity described for alpha smooth muscle actin in oral AML (1-2,4-6,10) and negativity for HMB-45 (1-2,4-6). Interestingly, our case was positive for desmin, which not occurred in the cases reported by Ide et al. (4) and Yamamoto et al. (10).
The differential diagnosis includes angiolipoma and angioleiomyoma. Angiolipoma is composed of blood vessels and fat tissue, and does not present smooth muscle proliferation. To differentiate angiomyolipoma from angiolipoma, it is necessary to demonstrate smooth muscle bundles. Angioleiomyoma may resemble AML, because both show abundant blood vessels and smooth muscle fibres. Furthermore, there are some angioleiomyomas reported in the literature that exhibited mature fat cells (10). The histopathology characteristics found in our case, excluded the differential diagnosis previously mentioned.
]]> In summary, we report an additional case of oral AML located in the upper lip. This case and the English-language literature data confirms that oral AMLs are uncommon, solitary, noninvasive, and easily resected lesions, rarely associated with TS, and negative for HMB-45.
References
1. Piattelli A, Fioroni M, Rubini C, Fiera E. Angiomyolipoma of the palate. Report of case. Oral Oncology 2001;37:323-5. [ Links ]
2. Foschini MP, Corti B, DaCol M, Cenzi M, Zanella MD, Barbazza R. Angiomyolipoma of the parotid gland: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:738-41.
3. Gutmann J, Cifuentes C, Vicuña R, Sobarzo V, Balzarini MA. Intraoral angiomyolipoma. Oral Surg 1975;39:945-8.
4. Ide F, Shimoyama T, Horie N. Angiomyolipomatous hamartoma of the tongue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:581-4.
5. Watanabe K, Toshimitsu S. Mucocutaneous Angiomyolipoma: a report of 2 cases arising the nasal cavity. Arch Pathol Lab Med 1999;123:789-92.
6. Ito M, Sugamura Y, Ikari H, Sekine I. Angiomyolipoma of the lung. Arch Pathol Lab Med 1998;122:1023-5.
7. Stout AP. Tumors of the tissue, section II, fascicle 5. In: Atlas of tumors pathology. Washington DC: Armed Forces Institute of Pathology; 1953. p. 61.
]]> 8. Shimizu M, Manabe T, Tazelaar HD, Hirokawa M, Moriya T, Ito J, et al. Intramyocardial angiomyolipoma. Am J Pathol 1994;18:1164-9.9. Val-Bernal JF, Mira C. Cutaneous angiomyolipoma. J Cutan Pathol 1996;23:364-8.
10. Yamamoto K, Nakamine H. Angiomyolipoma of the oral cavity: report of two cases. J Oral Maxillofac Surg 1995; 53: 459-61.
11. López JL, Campillo ERR, Soares MSM, Zubeldia FF, Küstner EC, Llabrés XR. Esclerosis tuberosa y manifestaciones orales. Caso clínico. Med Oral 2004;9:216-23.
 Correspondence:
Correspondence:
Dr Roman Carlos
Centro de Medicina Oral de Guatemala, 16 calle 4-53 zona 10
Edificio Marbella ]]>
Ciudad de Guatemala
Guatemala
E-mail: roman@guate.net.gt
Received: 24-12-2005
Accepted: 15-11-2006