Sporadic oral angiomyolipoma. Case report
Carlos Álvarez Alvarez1, Jacinto Fernández Sanromán2, Manuel Fernández Castilla3, Iosu Antón Badiola4
(1) M.D. Department of Pathology
(2) M.D. Department of Maxillofacial Surgery
(3) M.D. Department of Radiology
(4) M.D. Head of Department of Pathology
ABSTRACT
Angiomyolipoma (AML) is a rare, benign tumour composed of a variable proportion of lipocytes, smooth muscle and thick-walled blood vessels. AML is part of a family of tumours arising from perivascular epithelioid cells (PEComas), and many cases are associated with tuberous sclerosis, with the kidney being the most frequent site involved. We report a case of sporadic AML in the hard palate of a 52-year-old male, an extremely unusual location for this tumour. Differentiation from other benign and malignant oral mesenchymal lesions depends on recognition of the three histologic components, and immunohistochemical techniques may be helpful. AML occurring in the head and neck do not express HMB-45, an antibody that identifies immature melanosomes, conversely to the usual immunopositivity shown in AMLs from kidney and liver, suggesting that there are differences among them. A wide surgical excision is considered curative, as this tumour usually behaves in a benign fashion.
Key words: Angiomyolipoma, palate, HMB-45, angioleiomyoma.
RESUMEN
El angiomiolipoma (AML) es un tumor benigno infrecuente compuesto por una proporción variable de lipocitos, músculo liso y vasos de paredes gruesas. Forma parte de la familia de tumores originados en las células epitelioides perivasculares (PEComas), y muchos casos se asocian a esclerosis tuberosa, siendo el riñón la localización más frecuente. Presentamos un caso de AML esporádico en el paladar duro de un varón de 52 años, una localización extremadamente rara para este tumor. El diagnóstico diferencial con otras lesiones mesenquimales tanto benignas como malignas de la zona se basa en la identificación histológica de los 3 componentes, siendo de ayuda las tinciones inmunohistoquímicas. Los AMLs localizados en cabeza y cuello no expresan HMB-45, un anticuerpo que identifica melanosomas inmaduros, mientras que los renales y hepáticos sí lo hacen, lo que sugiere que existen diferencias entre ambos AMLs. El tratamiento de elección es la exéresis quirúrgica completa, ya que estos tumores suelen tener un comportamiento benigno.
Palabras clave: Angiomiolipoma, paladar, HMB-45, angioleiomioma.
]]> Introduction
Angiomyolipoma (AML) is a rare benign mesenchymal tumour that occurs most commonly in the kidney. Generally considered benign, it contains variable amounts of smooth muscle, adipose tissue and blood vessels. Some AML occur in the setting of tuberous sclerosis (TS), and others are sporadic cases (1,2). We present the clinical, radiographic, and pathologic findings of an AML of the hard palate in a 52-year-old man without TS, an extremely unusual location for this tumour. The correct diagnosis rests on identifying the triad of fat, vessels, and smooth muscle.
Case report
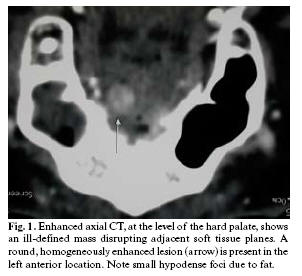
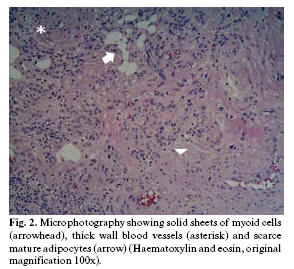
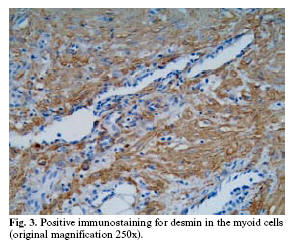
A 52-year-old male with no clinical evidence of TS noticed a small painless lump in the hard palate. Grossly, a 6-mm polypoid and reddish tumour was observed. Contrast-enhanced computed tomography (CT) showed an ill-defined, round, homogeneously enhanced lesion in the hard palate disrupting adjacent soft tissue planes, without lymphadenopathy (Fig. 1). A hemangiomatous lesion was suggested, and the tumour was widely excised. On microscopic examination the mucosa appeared bulged by a well-circumscribed but unencapsulated mass composed of an admixture of smooth muscle cells and thick-walled vessels. Irregularly dispersed among the smooth muscle cells were scarce adipocytes singly and in small clusters (Fig. 2). Smooth muscle cells stained positively for desmin (Fig. 3), muscle specific actin, and h-caldesmon, and adipocytes were positive for S-100 protein. No immunostaining was seen for cytokeratins or HMB45. Histopathological diagnosis was AML.
Discussion
]]> AML is considered part of a family of tumours arising from perivascular epithelioid cells (PEComas) that show co-expression for melanocytic and muscle markers (1). AML is the most common benign tumour of the kidney, and has been encountered less often in other locations, the liver being the most common. The most frequently reported sites in the head and neck region were the lips, the palate, and buccal mucosa (2-4).AML can occur in association with TS complex, or as an isolated disorder. In about half of the cases renal AMLs are associated with TS, and these tumours are often multiple, bilateral, and associated with cysts. In the oral cavity, only 11 cases, including the present one, have been reported, and only one of them was multiple and associated with TS (4). They differ from renal and hepatic AMLs in that they lack epithelioid cells (2,3,5) and are negative for the monoclonal antibody against immature melanosomes HMB-45 (2,4), conversely to the usual immunopositivity shown in AMLs from other sites (1).
Clinically, oral AML could be confused with any other exophytic tumour. AML seldom has been included in the differential diagnosis of a mass of the oral region before surgical excision, but preoperative radiological diagnosis of AML could be possible if intratumoral fat can be demonstrated. The presence of myoid cells, adipose tissue and blood vessels are the characteristic histopathological clues.
As the proportions of the components vary considerably from patient to patient, a careful search for adipocytes and abnormal blood vessels may help in the diagnosis because there may be scarce adipose tissue. Strongly positive smooth muscle actin and desmin immunostaining confirm the presence of smooth muscle. From a histological point of view, AML should be distinguished from angiolipoma and angioleiomyoma, which is an encapsulated tumour characterised by vascular spaces surrounded by thick smooth muscle walls. Although small groups of mature fat cells have been rarely reported in some angioleiomyomas, these tumours tend to occur in women, whereas AMLs usually affect older men and are unencapsulated tumours.
A wide surgical excision is considered curative, as this tumour usually behaves in a benign fashion (2-5).
References
1. Eble JN. Angiomyolipoma of kidney. Semin Diagn Pathol 1998;15:21-40 [ Links ]
2. Watanabe K, Suzuki T. Mucocutaneous angiomyolipoma. A report of 2 cases arising in the nasal cavity. Arch Pathol Lab Med 1999;123:789-92. [ Links ]
3. Piattelli A, Fioroni M, Rubini C, Fiera E. Angiomyolipoma of the palate. Report of a case. Oral Oncol 2001;37:323-5. [ Links ]
4. López-López J, Rodríguez de Rivera E, Marqués MS, Finestres F, Chimenos E, Roselló X. Tuberous sclerosis and its oral manifestations. A clinical case. Med Oral 2004;9:216-23 [ Links ]
5. Tardio JC, Martin-Fragueiro LM. Angiomyolipoma of the nasal cavity Histopathology 2002;41:174-5. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Carlos Alvarez Alvarez
Servicio de Anatomía Patológica. Hospital Montecelo
Mourente s/n
36071 Pontevedra.España
E-mail: capialvarez@yahoo.com