










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 no.2 Madrid feb. 2010
Pyogenic versus amoebic liver abscesses. A comparative clinical study in a series of 58 patients
Absceso hepático piógeno versus amebiano. Estudio clínico comparativo de una serie de 58 casos
A. Cosme1, E. Ojeda2, I. Zamarreño2, L. Bujanda1, G. Garmendia3, M. J. Echeverría4 and J. Benavente2
1Gastroenterology Department. Donostia Hospital. CIBEREHD. University of the Basque Country. San Sebastián, Guipúzcoa. Spain. Departments of 2Internal Medicine, 3Radiology, and 4Microbiology. Donostia Hospital. San Sebastián, Guipúzcoa. Spain
ABSTRACT
Objective: to compare the clinical and epidemiological characteristics of patients with pyogenic liver abscess (PLA) and with amebic liver abscess (AHA) in order to determine the potential factors that may help improve diagnosis and treatment for this disease.
Material and method: a retrospective study of clinical histories of 45 patients with PLA and 13 with ALA, diagnosed between 1985 and 2005 in Donostia Hospital in San Sebastián.
Results: among the 45 patients with PLA (30 men and 15 women, with a mean age of 61 years and 11 months), more than a half were cholangitic (13 cases) or were of unknown origin (15 cases). In 10 patients, diabetes was considered to be a predisposing condition. Increased ESR (> 30), leukocytosis (> 12,000), fever and abdominal pain were observed in 95.5%, 86.7%, 82.8% and 68.9%, respectively. Twenty-five patients had single abscesses. Abscess and blood cultures were positive in 77.1% and 50% of cases, respectively (44.4% with polymicrobial infection). E. coli and S. milleri were the most commonly found germs. A percutaneous drainage was performed on 22 patients. Mean hospital stay was 27 days, and overall mortality, including that related to concomitant conditions, was 7 of 45 cases.
Of the 13 cases of ALA (7 men and 6 women, with mean age of 42,9 years), 2 were locally acquired. Increased AF and GGTP (> 2N), fever, leukocytosis and ESR (> 30) were observed in 92.3, 77, 70 and 61.5% of cases, respectively. There were single abscesses in 10 patients and all except one were located in the right lobe. The serological test for E. histolytica (IFF ≥ 1/256) was positive in 100% of cases. A percutaneous drainage was carried out on 6 patients. Mean hospital stay was 18 days and two patients died.
Conclusions: In our series, the clinical parameters suggesting pyogenic origin were: age 50 or older, male gender, diabetes, moderately elevated bilirubin and transaminases. In amoebic cases the associated features were being aged 45 or younger, diarrhoea, and presence of a single abscess in the right lobe. Parasitism by E. histolytica must be considered in the differential diagnosis of liver abscesses, even with no epidemiological clinical history of travel and/or immigration.
Key words: Liver abscess. Pyogenic. Amoebic. Comparison.
RESUMEN
Objetivo: comparar las características clínicas y epidemiológicas de los pacientes con absceso hepático piógeno (AHP) y con absceso hepático amebiano (AHA) para establecer posibles factores que ayuden a mejorar el diagnóstico y tratamiento de la enfermedad.
Material y método: se realiza un estudio retrospectivo de las historias clínicas de 45 pacientes con AHP y de 13 con AHA, diagnosticados entre 1985 y 2005 en el Hospital Donostia de San Sebastián.
Resultados: de los 45 casos de AHP (30 hombres y 15 mujeres con una edad media de 61 años y 11 meses), más de la mitad fueron de origen colangítico (13 casos) o criptogenético (15 casos). La diabetes como enfermedad predisponente se objetivó en 10. La elevación de la VSG (> 30), leucocitosis (> 12.000), fiebre y dolor abdominal se observaron en el 95,5, 86,7, 82,8 y 68,9% de los casos respectivamente. Los abscesos fueron solitarios en 25 casos. Los cultivos del absceso y los hemocultivos fueron positivos en el 77,1 y 50%, respectivamente (44,4% de los casos eran polimicrobianos). E. coli y S. milleri fueron los gérmenes más habituales. Se hizo drenaje percutáneo en 22 pacientes. La mortalidad global, incluida la relacionada con la patología subyacente, fue de 7 casos y la estancia media hospitalaria de 27 días.
De los 13 casos de AHA (7 hombres y 6 mujeres con una edad media de 42 años y 9 meses), 2 fueron autóctonos. La elevación de la FA y GGTP (> 2N), fiebre, leucocitosis y VSG (> 30) se observaron en el 92,3, 77, 70 y 61,5% de los casos respectivamente. Los abscesos fueron únicos en 10 casos y excepto uno, 12 se localizaron en el lóbulo derecho. La serología a E. histolytica (IFI ≥ 1/256) fue positiva en el 100% de los casos. Se hizo drenaje percutáneo en 6 pacientes. La mortalidad fue de 2 casos y la estancia media hospitalaria de 18 días.
Conclusiones: en nuestra serie, las características clínicas que sugieren un origen piógeno son: la edad superior a 50 años, el sexo masculino, la diabetes y la bilirrubina y transaminasas moderadamente elevadas. En el amebiano, la edad menor de 45 años, la diarrea y la localización solitaria del absceso en el lóbulo derecho. La parasitación por E. histolytica se debe considerar en el diagnóstico diferencial de los abscesos hepáticos, incluso sin el antecedente epidemiológico de viajes o de inmigración.
Palabras clave: Absceso hepático. Piógeno. Amebiano. Comparación.
Introduction
The incidence of pyogenic liver abscess (PLA) ranges from 1.1 to 2.3 cases per 100,000 population every year (1,2). PLA occurs mainly in immunosuppressed and diabetic patients, and in individuals suffering from malignant neoplasia. Its prevalence has increased in recent years due to liver transplantation. Clinical characteristics depend on the pathogenic mechanism involved. Mortality rates have been reported as 6-32% in various hospital series (2,3).
Parasitism by Entamoeba histolytica in developed countries occurs in specific population subgroups: immigrants and travellers coming from endemic regions, psychiatric hospital patients, individuals with occasional contact with people coming from areas with amoebiasis, and those who have ingested contaminated food. The prevalence of infection by E. histolytica in Spain is low: 0.7% in the Barcelona hospital population (1978) (4), a percentage of 1.79% in a population in the northern area of Huelva province (1998) (5), and between 2.2 to 21% in adult immigrants (2002) (6). Mortality rates range from less than 1% in patients with abscesses without complications to 34% in complicated cases (7). The approximate incidence of amoebic liver abscess (ALA) in Guipuzcoa is of 0.1 cases for every 100,000 people every year.
In this study, liver abscess cases are reviewed retrospectively to establish the clinical differences between the pyogenic and amoebic aetiologies, thereby facilitating early treatment in these patients. Some of these cases have been the subject of prior reviews and communications (8,9).
Patients and method
The clinical histories of patients diagnosed with PLA and ALA between 1985 and 2005 in Donostia Hospital, San Sebastián, were reviewed retrospectively.
Pyogenic liver abscess was defined as the observation of one or more ultrasound and CT images with positive cultures, or by positivity in two or more blood cultures of germs consistent with the diagnosis. Hepatic lesions diagnosed by imaging techniques, but without positive cultures of the pus, were included after ruling out other diseases according to the clinical history. An amoebic aetiology was demonstrated by serology (antibody titre against E. histolytica by IIF ≥ 1/256), faeces and/or abscess culture, and by location in the liver by imaging techniques.
The following variables were taken into account: age, sex, clinical features, blood and other diagnostic tests, type of abscess and location within the liver, treatment, evolution, and average hospital stay in both series. In addition, predisposing diseases and the origin of abscesses for pyogenic abscesses (45 cases), and associated diseases, epidemiological history of travelling to areas with a high prevalence of amoebiasis, the origin of patients, and the time between having been to endemic areas and the occurrence of symptoms in amoebic cases (13 cases) were analysed.
Statistical analysis
In order to evaluate the differences between demographic data for PLA and ALA, the chi square test and/or Fisher's test were used for categorical variables, and Student's t-test and the non-parametric Mann-Whitney U test for quantitative variables. Differences between groups were considered to be significant when p value was less than 0.05.
Results
During the two decades studied, 45 patients were diagnosed with PLA caused by bacteria, and there were 13 cases of ALA. The clinical features and laboratory data of the two series are shown in table I. Predisposing conditions for pyogenic abscesses were: diabetes mellitus (10 cases); tumours (4, out of which 2 had liver metastasis); chronic pancreatitis (4); hydatid cysts; (3) infection by HIV (1); and liver cirrhosis (1). The origin of the abscess was biliary in 13 cases, phlebitis of the portal vein in 5, spread of infection from previous liver lesions in 5, haematogenic in 4, by contiguity in 3, and 15 of unknown origin.
The clinical history of patients with amoebic abscesses included: malaria, chronic liver disease due to hepatitis B and C viruses (1 case), and chronic obstructive pulmonary disease COPD (1 case). Eleven out of thirteen lived in Guipuzcoa, one lived in Uruguay (was on holiday in Guipuzcoa), and another came from Japan (but had been living in Guipuzcoa for the previous 6 months). Eleven had travelled to areas where the disease is endemic -India (4), Mexico (3), Costa Rica, Uganda, Guinea and Morocco (1)-. In 82% of cases symptoms appeared within the first 5 months after the visit. Two individuals did not have any history of exposure to endemic areas. One of them may have been infected by their partner who suffered from amoebic colitis, and the other one had a risk factor due to his/her profession (drain cleaner). Concomitant amoebic colitis was present in 5 patients.
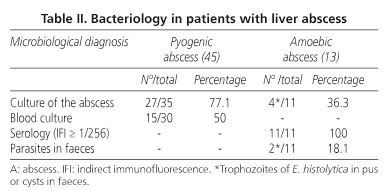
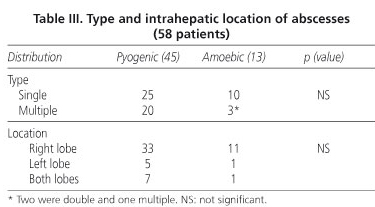
Microbiological diagnoses and findings from imaging techniques for the 58 patients studied are shown in tables II and III. Abdominal echography was performed on 50 patients, leading to a diagnosis in 38 (76%), while a CT scan was carried out on 55, and a diagnosis was reached in 96% of these cases (Fig. 1). The micro-organisms isolated from the pyogenic abscesses were: aerobic gram negative rods (23 cases), anaerobic bacteria (15), aerobic gram positive cocci (14), aerobic gram positive rods (1) and Brucella (1). A total of 44.4% (12 out of 27) of abscesses with a bacteriological diagnosis were polymicrobial. E. coli and S. milleri (21 cases) were the most commonly found germs. Amoebic abscesses were larger than 10 cm in diameter in 5 cases (4 single and 1 multiple), and larger than 5 cm in a further 7 cases (5 single and 2 multiple).

The treatment of patients with PHA consisted of antibiotherapy, drainage and surgery. The most commonly used antibiotic combination were third generation cephalosporins with metronidazole, alone or with aminoglycosides (17 cases), imipenem or piperacillin-tazobactam (16), and aminoglycosides with metronidazole (5). Antibiotic therapy without drainage was carried out in 10 patients (one recurred and needed surgery due to biliary stenosis). CT-guided percutaneous drainage in association with adequate antibiotic coverage was used in 22 patients (Table IV). This procedure was successful in 18 (full recovery 81.8%). In 13 patients, where the drainage was not successful, surgery was undertaken. Overall mortality was related to the diseases that needed surgical treatment (acute cholecystitis, obstructive icterus, infected hydatid cyst in the liver, peritonitis, postoperative biliary stenosis, and carcinoma of the gallbladder). The average hospital stay of those patients who were treated with percutaneous drainage was shorter than that of those treated with surgery (21 versus 40 days).

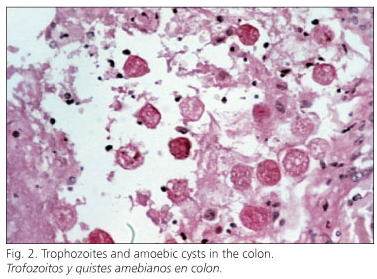
Patients suffering with ALA were treated with metronidazole and paramomycin as a first choice. CT-guided percutaneous drainage was carried out in 6 cases (5 of them with abscess sizes exceeding 10 cm), and surgery in 4 cases. Mortality rates and mean hospital stay are shown in table IV. Two people died; one due to peritonitis secondary to multiple perforations in the colon due to amoebic ulcerative colitis (Fig. 2) in association with septic shock, and the other one due to large multiple abscesses with sepsis and respiratory distress.
Discussion
Amoebiasis is a protozoan disease that affects 10% of the world population with a high prevalence in Mexico and South Africa (among the black population), some areas in the Middle East, South and Southeast Asia, and parts of Western Africa and South America. ALA occurs in between 3 and 9% of the people infected with the parasite. In Spain, during the last decade, there has been an increase in the number of autochthonous cases. Some series of patients suffering from ALA have indicated a predilection for middle-aged men, and that it is less common at extreme ages (10-13).
PHA has a variable occurrence in the population according to concomitant diseases. The risk of developing a pyogenic abscess in diabetic people and in those suffering from malignant tumours is tenfold higher than that of the general population; in patients who have undergone liver transplantation it is 445 times higher (2). PHA often occurs in individuals over 50 years old with a slight predominance in men (14,15). Abscesses secondary to ascending cholangitis and of unknown origin are the most common.
ALA is caused by the colonization of the liver by trophozoites of pathogenic strains of E. histolytica through portal circulation. It causes foci of necrosis in the liver parenchyma, most of the time leading into a single cavity. The most common clinical signs and symptoms are abdominal pain (70-100 of the cases) in association with fever (70-100%) and diarrhoea, with or without blood (30-50% of the cases). Sometimes, the abscess only causes fever.
The classical symptomatology of PLA (fever, shivering, and pain in the lower right abdomen with or without hepatomegaly, of subacute presentation), occurs in a small percentage of patients. In recent Spanish series (9,16-20), up to 60% of patients lack symptoms suggestive of processes in the lower right abdomen. Icterus is often associated with biliary pathology. Table V shows the differential characteristics of PLA and ALA from other studies in Central and South American and Asian countries (14,15,21-24).
Blood tests for both types of abscesses are similar: increased ESR, leukocytosis with left shift, and slight changes in liver function tests. In cases secondary to biliary tract infection, bilirubin levels are often increased. In blood tests in amoebic infections there is often a moderate increase of alkaline phosphatase; icterus is rare and, when present, moderate.
Abdominal contrast CT is the technique of choice for the diagnosis of liver abscesses. In our series, it helped in the diagnosis of lesions in 96% of patients, similar to what is reported in the literature (3,9,12,23,25,26). Its sensitivity is almost 100% higher than echography, which remains the first examination to be carried out because of its low cost and ready availability. However, both CT scans and echography may lead to false negatives in abscesses smaller than 1 cm in diameter, in those located near the diaphragmatic dome, and in those in early stages of development.
The microbiological diagnosis of pyogenic abscesses is based on the identification of the germ by culture, with samples obtained from the liver by FNA -70-95% of cases (9,15-20,23)-, or by blood culture -40-60% of cases (9,15-20,23)-. In amoebic abscesses several methods were used: detection of specific antigens (adhesine Gal-GalNac) and serum antibodies against E. histolytica, fecal smear test, FNA of abscesses, and molecular biology techniques. Of these, the serological test (indirect hemaglutination) is the most sensitive (positive in 90-100% of the cases), while faecal smear test and microbiological culture are least affordable. PCR is considered the gold standard for immigrants coming from endemic areas and frequent travellers who carry antibodies against E. histolytica for several years after being infected. Currently, a very specific technique which can be used for the diagnosis of ALA as long as the subject has not been treated with amoebacides is the presence of adhesin Gal-GalNac in the serum (27).
The treatment of choice for PLA (echo or CT-guided percutaneous drainage in association with antibiotics) cures between 72 and 90% of patients, with complications ranging from 4 to 18% (28-30). The absolute contraindications for guided drainage are when there is an indication for surgery because of an associated disease or significant coagulopathy. Relative contraindications are ascites, very viscous purulent material, multiple small abscesses, and the risk of damaging vital structures, especially those in the left lobe. Surgery is performed when percutaneous treatment fails, or there are absolute or relative contraindications for guided drainage, associated diseases secondary to surgical treatment, or abscesses with rupture or haemorrhage. Antibiotic treatment without drainage is controversial. It should be applied only in patients with small abscesses and always considering each individual case (9,28). In our series, such diverse treatments are explained by the fact that patients were seen at different points over a long period (20 years).
The treatment for ALA consists of the intraluminal and systemic administration of amoebacides as soon as possible. Guided percutaneous drainage is performed in case of large abscesses (> 8 cm) (31), those located in the left lobe, and when there is no response to medical treatment or liver failure is present. There is no current evidence whether guided percutaneous drainage provides extra benefits compared to treatment with metronidazole alone in uncomplicated ALA cases (32). Surgical treatment is performed if percutaneous drainage fails or complications arise. Mortality rates are lower than 1% in uncomplicated cases (without superinfection or rupture to the peritoneum, pleura or pericardium).
The limitations of this study are its retrospective, observational nature, and that it includes a relatively small number of cases compared to other Central and South American Asian studies. However, it represents one of the few series in our country (12) in which the clinical pictures of these two types of liver abscesses are compared.
As a conclusion, in our series PLA occurred in people aged 50 or over, often with diabetes, and generally associated with bilirubin levels over 2 mg/dL. On the other hand, subjects with ALA had an epidemiological history of travel or immigration. Diarrhoea was one of the initial symptoms of the disease, and they had a single abscess predominantly in the right lobe.
References
1. Hansen PS, Schonheyder HC. Pyogenic hepatic abscess: a ten year population-based retrospective study. APMIS 1998; 106: 396-402. [ Links ]
2. Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin Gastroenterol Hepatol 2004; 2: 1032-8. [ Links ]
3. Cosme Jiménez A, Bujanda Fernández de Piérola L, Ojeda Pérez E. Abscesos hepáticos piógenos. El especialista opina. Disponible en: http://www.nacom.es/Med1/3/doc/expertodocumentos/2001. [ Links ]
4. Portús M, Prats G. Contribución al conocimiento de las protozoosis intestinales en la población hospitalaria barcelonesa. Med Clin (Bar) 1981; 76: 203-5. [ Links ]
5. Perea R, Bassas E, Lepe JA, Lombardo M, Garcés M. Prevalencia de anticuerpos frente a Entamoeba histolytica en la zona norte de la provincia de Huelva. Med Clin (Bar) 1998; 110: 275. [ Links ]
6. Pérez Arellano JL, Muro Álvarez A, Hernández Cabrera M, Martín Sánchez AM. Amebosis. Medicine (Madrid) 2002; 8: 3731-41. [ Links ]
7. Ortiz FM, Devesa F, Ferrando J, Ferrando I, Borghol A, Gutiérrez J. Absceso hepático amebiano: ¿tratamiento farmacológico o punción-aspiración? Gastroenterol Hepatol 2007; 30: 399-401. [ Links ]
8. Pérez Trallero E, Cilla Eguiluz G, Urbieta Egaña M, Muñoz Baroja I. Infecciones autóctonas por Entamoeba histolytica. Med Clin (Bar) 1985; 85: 254. [ Links ]
9. Barrio J, Cosme A, Ojeda E, Garmendia G, Castiella A, Bujanda L, et al. Abscesos hepáticos piógenos de origen bacteriano. Estudio de una serie de 45 casos. Rev Esp Enferm Dig 2000; 92: 232-5. [ Links ]
10. Djossou F, Malvy D, Tamboura M, Beylot J, Lamouliatte H, Longy-Boursier M, et al. Amoebic liver abscess. Study of 20 cases with literature review. Rev Med Inter 2003; 24: 97-106. [ Links ]
11. García-Forcada A, Sans M, Gascon J, Valls ME, Bru C, Corachan M. Absceso hepático amebiano: revisión de 13 casos. Med Clin (Bar) 1995; 105: 537-40. [ Links ]
12. Blanco Quintana F, Novellas Arribas B, Sánchez Molini P, Sanz Sanz J. Descriptive study of 39 cases of hepatic abscess of pyogenic and amebic origin. An Med Interna (Madrid) 1995; 12: 477-84. [ Links ]
13. Nari GA, Ceballos Espinosa R, Carrera Ladrón de Guevara S, Preciado Vargas J, Cruz Valenciano JL, Briones Rivas JL et al. Abscesos amebianos de hígado. Tres años de experiencia. Rev Esp Enferm Dig 2008; 100: 268-72. [ Links ]
14. Barbour GL, Juniper K. A clinical comparison of amebic and pyogenic abscess of the liver in sixty-six patients. Am J Med 1972; 53: 323-34. [ Links ]
15. Conter RL, Pitt HA, Tompkins RK, Longmire WP. Differentiation of pyogenic from amebic hepatic abscess. Surg Gynecol Obstr 1986; 162: 114-20. [ Links ]
16. Comas P, Vargas V, Almirante B, González A, García D, Esteban R, et al. Absceso piógeno hepático. Revisión de 33 casos. Rev Clin Esp 1989; 185: 225-30. [ Links ]
17. Corbella X, Vadillo M, Torras J, Pujol M, Rafecas A, Gudiol F. Presentación, diagnóstico y tratamiento del absceso hepático piógeno: análisis de una serie de 63 casos. Enferm Infecc Microbiol Clin 1995; 13: 80-4. [ Links ]
18. Ramos A, Gazapo T, Murillas J, Martín H, Mandaza P, Cuervas V. Absceso hepático piógeno. Estudio descriptivo de 35 casos. Gastroenterol Hepatol 1996; 19: 292-6. [ Links ]
19. Asensi V, Rodríguez A, Carton JA, Maradona JA, Álvarez E, Llera JM, et al. Abscesos hepáticos piógenos. Revisión de 59 casos y experiencia con imipenem. Rev Clin Esp 1997; 197: 494-9. [ Links ]
20. Jiménez E, Tiberio G, Sánchez J, Jiménez FJ, Jiménez G. Abscesos hepáticos piógenos: experiencia de 16 años en su diagnóstico y tratamiento. Enferm Infecc Microbiol Clin 1998; 16: 307-11. [ Links ]
21. Ogden WW, Hunter PR, Rives JD. Liver abscess. Postgrad Med 1961; 30: 11-9. [ Links ]
22. May RP, Lehmann JD, Sanford JP. Difficulties in differentiating amebic from pyogenic liver abscess. Arch Intern Med 1967; 119: 69-74. [ Links ]
23. Barnes PF, De Cock KM, Reynolds TN, Ralls PW. A comparison of amebic and pyogenic abscess of the liver. Medicine (Baltimore) 1987; 66: 472-83. [ Links ]
24. Lodhi S, Sarwari AR, Muzammil M, Salam A, Smego RA. Features distinguishing amoebic from pyogenic liver abscess: a review of 577 adult cases. Trop Med Int Health 2004; 9: 718-23. [ Links ]
25. Greenstein AJ, Barth J, Dicker A, Bottone EJ, Aufses AH. Amebic liver abscess: a study of 11 cases compared with a series of 38 patients with pyogenic liver abscess. Am J Gastroenterol 1985; 80: 472-8. [ Links ]
26. Ahsan T, Jehangir MU, Mahmood T, Ahmed N, Saleem M, Shahid M, et al. Amoebic versus pyogenic liver abscess. J Pak Med Assoc 2002; 52: 497-501. [ Links ]
27. Haque R, Mollah NU, Ali IK, Alam K, Eubanks A, Lyerly D, et al. Diagnosis of amebic liver abscess and intestinal infection with the TechLab Entamoeba histolytica II antigen detection and antibody tests. J Clin Microbiol 2000; 38: 3235-9. [ Links ]
28. Seeto RK, Rockey DC. Pyogenic liver abscess. Changes in etiology, management and outcome. Medicine (Baltimore) 1996; 75: 99-113. [ Links ]
29. Bru C, Ayuso MC, Bianchi L, De la Torre P, Texeidor N. Abscesos hepáticos: drenaje percutáneo bajo control ecográfico. Gastroenterol Hepatol 1986; 9: 15-20. [ Links ]
30. Eroles G, Mecina AB, Fernández C, Mancebo AB, Riva L. Abscesos hepáticos: revisión retrospectiva de 68 casos. An Med Interna (Madrid) 2008; 5: 335-41. [ Links ]
31. Graillet R, Sánchez-Aguilar M, Morán-Mendoza AO, Hernández-Sierra JF, Gordillo-Moscoso A, Tapia-Pérez JH. Análisis de factores asociados al fracaso del tratamiento médico del absceso hepático amebiano. Cir Esp 2008; 84: 83-6. [ Links ]
32. Chavez-Tapia NC, Hernández-Calleros J, Tellez-Avila FI, Torre A, Uribe M. Image-guided percutaneous procedure plus metronidazole versus metronidazole alone for uncomplicated amoebic liver abscess (Review). Cochrane Database Syst Rev 2009; 21(1): CD004886. [ Links ]
![]() Correspondence:
Correspondence:
Ángel Cosme Jiménez.
Servicio de Aparato Digestivo.
Hospital Donostia.
Paseo Dr. Beguiristain, s/n. 20014 San Sebastián.
email: acosme@chdo.osakidetza.net
Received: 01-04-09.
Accepted: 28-10-09.

