










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.4 Madrid abr. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Enteral stent for the treatment of a urinary fistula associated with a biological mesh following a Bricker-type procedure
Tratamiento mediante prótesis enteral de una fístula urinaria asociada a malla biológica tras una cirugía tipo Bricker
Raquel Díaz-Ruiz, Marta Castillo-Pradillo, Óscar Nogales-Rincón and Cecilia González-Asanza
Department of Digestive Surgery. Hospital General Universitario Gregorio Marañón. Madrid, Spain
Introduction
Postoperative fistula results in increased morbidity and a longer hospital stay. While surgery is the most common treatment, the endoscopic approach (1) is an increasingly used alternative (2).
Case report
A 57-year-old woman underwent surgery for colonic adenocarcinoma, which relapsed as peritoneal carcinomatosis and was managed with chemotherapy and surgery; a biological Permacol™ mesh was used for abdominal wall closure. In 2015 she relapsed again at the recto-vesical pouch with infiltration of the rectum, bladder, and vaginal dome. She underwent pelvic exenteration with vaginoplasty and Bricker-type urinary diversion across the mesh. During the postoperative period an ileal loop urinary fistula was seen, secondary to mesh decubitus. An endoscopy of the Bricker loop was performed, which revealed a fistulous orifice with a whitish background at 7 cm from the mesh-related ileostomy, which took up 50% of the perimeter (Fig. 1). Endoscopic placement of a 100 mm x 20 mm covered metal stent (Hanarostent® Colon/Rectum) was decided upon (Fig. 2), which was uneventfully removed after 12 weeks, whereupon fistula healing was accomplished (Fig. 3).


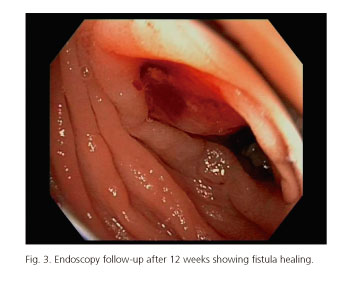
The stent was fitted for a longer period than recommended, due to our experience and the fistula size. Despite a potential relapse risk from mesh persistence, the patient remains free of recurrence, likely due to perifistular fibrosis formation.
Discussion
Complex fistulas at atypical locations may be managed with endoscopically placed metal stents, thus preventing repeated surgery (3).
References
1. Mangiavillano B, Pagano N, Arena M, et al. Role of stenting in gastrointestinal benign and malignant diseases. World J Gastrointest Endosc 2015;7:460-80. [ Links ]
2. Lamazza A, Sterpetti AV, De Cesare A, et al. Endoscopic placement of self-expanding stents in patients with symptomatic anastomotic leakage after colorectal resection for cancer: Long-term results. Endoscopy 2015;47:270-2. DOI: 10.1055/s-0034-1391403. [ Links ]
3. Montes López C, Romeo Martínez JM, Tejero Cebrián E, et al. Tratamiento de la estenosis neoplásica de colon izquierdo mediante la colocación de prótesis autoexpandibles. Rev Esp Enferm Dig 2001;93:226-31. [ Links ]
