










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkArchivos Españoles de Urología (Ed. impresa)
versión impresa ISSN 0004-0614
Arch. Esp. Urol. vol.62 no.2 mar. 2009
Single prostatic metastasis of a small cell lung carcinoma
Metástasis única en próstata de carcinoma microcítico pulmonar
Isabel González Yañez1, Ma Eva Pérez López, José Ángel Rodríguez Lopez2, Ma Dolores Arias Santos3, Jesús García Gómez and Jesús García Mata
Medical Oncology1 and Pathological Anatomy3 Services. Orense Hospital.
Medical Oncology and Pathological Anatomy2 Services. Valdeorras Comarcal Hospital. Orense. Spain.
SUMMARY
Objective: To make the difference between two uncommon entities, small cell prostate carcinoma and prostatic metastasis of small cell lung cancer.
Methods/Results: We describe a case of single extra-pulmonar metastasis in the prostate from small lung carcinoma.
Conclusion: Clinical and radiographic findings and inmunohistochemistry allow differential diagnosis.
Key words: Small cell carcinoma. Prostate Metastases. Oat-cell carcinoma.
RESUMEN
Objetivo: Diferenciar dos entidades infrecuentes, carcinoma prostático de células pequeñas y metástasis prostática de tumor pulmonar de células pequeñas.
Métodos/Resultados: Presentamos un caso de carcinoma pulmonar microcítico con una metástasis única extra-pulmonar en la próstata, no descrito anteriomente.
Conclusiones: Los hallazgos clínicos y radiológicos si existen, y las técnicas de inmunohistoquímica permiten el diagnóstico diferencial.
Palabras clave: Carcinoma de celulas pequeñas. Metástasis prostática. Carcinoma microcítico.
Introduction
Neoplastic involvement of the prostate fundamentally occurs due to primary tumors originating in the same gland. Adenocarcinoma represents 95% of all cases, while small cell carcinoma, squamous carcinoma and transitional cell carcinoma have an incidence of less than 2% respectively. Similarly, prostatic metastases of a solid tumor are extremely rare and their findings are anecdotal.
Small cell or oat-cell lung tumors are generally associated with an aggressive course and have a large spread possibility. Hematogenous dissemination is the main propagation pathway. Any organ may be a potential target for malignant cells, but it is more likely to occur in the same lung, pleura, liver, bone, adrenal glands or the central nervous system (CNS). The appearance of a solitary prostatic metastasis without visceral or bone disease has not been described in the revised literature. It is difficult to differentiate from primary small cell carcinoma of the gland, which is fundamentally evaluated in a clinical context by means of immunohistochemistry on the biopsy.
We provide the case of a patient diagnosed with a small cell lung tumor with a solitary metastasis in the prostate, its treatment, obtaining a complete prostatic response by biopsy and its clinical evolution.
Case report
Patient aged 64 years without known allergies to medication, who had the following personal history: prostatic syndrome with normal prostate-specific antigen (PSA), recurrent paroxysmal atrial fibrillation and repeating nephritic colic. Smoker of more than 20 packets / year.
The patient was examined in the emergency service of the reference hospital for a clinical condition of back pain (similar to previous episodes of renal colic) and rapid atrial fibrillation in January 2007. In the chest X-ray condensation was observed in the lower right lobe with air bronchogram and widening of the mediastinum. The study was completed by conducting a computerized axial tomography (CAT) of the chest, which detected a mass in the previously described area with pathologic subcarinal adenopathy and ipsilateral pleural effusion of little volume. The bronchoscopy that was conducted subsequently showed a protrusion in the left main bronchus. The biopsy that was taken was diagnostic of "small cell lung carcinoma".
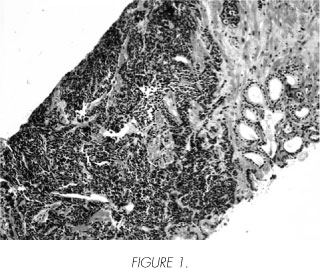
Before providing specific chemotherapy treatment, the extension study of the disease was conducted: normal cerebral nuclear magnetic resonance, normal bone scan (BS) and for tumor markers, the prostate-specific antigen (PSA) was the only elevated value (14.9). A prostatic biopsy was then conducted in February 2007, which showed the involvement of one of the three samples of the right prostatic lobe, whose histology was "undifferentiated small cell carcinoma consistent with lung tumor metastasis"; the left lobe was normal (Figures 1 and 2).

Therapy with carboplatin and etoposide started on the same month, 6 cycles being administered until June 2007, the 4th and 5th cycles including radiotherapy with radical intent on the lung mass and the mediastinum. A reduction of the PSA was observed in March 2007 (10.5). The toxicity was acceptable developing grade I esophagitis and grade I pneumonitis. Reviews started after the end of treatment.
The patient was assessed again in the urology service in December 2007, a new increase of the PSA being detected (14.6). As a result another prostatic biopsy was taken using ultrasound. This biopsy was found to be benign.
In the re-evaluation CAT of February 2008, nodes in the right and left adrenal glands were found. The study was completed with nuclear magnetic resonance (NMR), which confirmed progression of the disease in the adrenal glands, kidneys, pancreas and thoracic vertebrae T11 and T12. Acute renal failure (creatinine: 3.4) secondary to bilateral ureterohydronephrosis was found in the analysis. After right percutaneous nephrostomy, which improved renal function, 2nd line chemotherapy with topotecan started. Progression in the pancreas, adrenal glands, both kidneys and the abdominal wall was noted after three cycles. A new line of treatment with epirubicin started on August 2008. The disappearance of the lung and pleural metastatic lesions was observed in the latest re-evaluation CAT (October 2008), with the regression of the disease in the other sites. The PSA levels were found to be within the normal range.
Discussion
Small cell prostatic carcinoma belongs to 5% of neoplasms that are different from the common adenocarcinoma of the prostatic acini. It is very rare with less than 200 cases described in the literature. In the same way as in other sites, it has a high potential for being malignant and may produce paraneoplastic syndromes of ectopic hormonal secretion (Cushing's syndrome, Eaton-Lambert syndrome) (1).
On the other hand, lung cancer is the main cause of death due to malignancy in males. The histological variety of small or oat cell cancer is the most aggressive form. Patients with this lung tumor reach a progression free survival of approximately 5 months and an overall survival of almost 10 months. The metastasis can spread to any organ, but it is more likely to occur in the same lung, pleura, liver, bone, adrenal glands (2) or the CNS. The appearance of a solitary extrathoracic prostatic metastasis, like the case in question, without visceral or bone disease has not been described in the revised literature (3,4).
Small cell extrapulmonary neoplasms may be organ-confined (the most common are the gastrointestinal tract and the cervix) or disseminated (3). Progression free survival is approximately 7 months and overall survival can reach up to 32 months. Although the figures are discouraging, it is one of the differences in relation to the tumor originating in the lungs. They also show a lower percentage of metastases in the CNS and have a lower proportion of smokers among affected patients (4). Small cell prostatic tumors have a large potential to spread. It is normal to find a large prostatic mass and the presence of metastases during diagnosis due to the high probability of spreading and rapid tumor growth (1). The prostatic neoplastic involvement (metastatic, not primary) in this case was only described in one of the three samples of the right lobe obtained by biopsy. The therapeutic management of the small cell prostatic carcinoma does not differ if the disease is metastatic from the start, from the originator tumor in the respiratory tree. If the disease is confined to the prostate, surgery and/or radiotherapy are mandatory (5).
According to certain authors, initially there may be an increase of LDH (lactate dehydrogenase) and a decrease of serum albumin, which could be prognostic factors (6). Histologically, most show neuroendocrine differentiation that may be revealed by means of an immunohistochemical study. Neuron specific enolase (NSE) is generally positive; however, the PSA usually only shows reactivity when it coexists with adenocarcinoma. As such, hormonal therapy should also be included (1). The NSE was negative for our patient and no hormonal block was added when another PSA increase was determined after chemotherapy, after finding that the biopsy was benign. Response to the 3rd line of chemotherapy with the normalization of the PSA was also confirmed.
All these divergences, together with the existence of an already-known lung carcinoma allowed us to conduct the diagnosis of a prostatic metastasis of the same (never described previously in the literature as a solitary extra-pulmonary metastasis), resulting in a differential diagnosis that excluded a small cell prostatic tumor (7).
Immunohistochemistry is essential in difficult-to-determine cases. There is reactivity to cytokeratin CAM 5.2 and the NSE in the primary prostatic origin and the metastatic carcinoma originating in the lung. However, the former shows negative TTF-1 (thyroid and pulmonary transcription factor-1), but this is positive in the latter (1).
Conclusions
Prostatic small cell primary neoplasms are very rare. However, the solitary extrapulmonary metastatic involvement of this gland is even rarer, never having been reported until today. The differential diagnosis in our case has been easy due to the existence of a known lung cancer. In difficult cases, immunohistochemical measurements must be made. The prognosis seems to be bad in both cases, but it is also discouraging as this is a metastatic disease.
 Correspondence:
Correspondence:
Ma Eva Pérez López
Servicio de Oncología Médica
Complejo Hospitalario de Ourense
Ramón Puga, 52-54
32005 Orense. (Spain).
mevaplo@hotmail.com
maria.eva.perez.lopez@sergas.es
Accepted for publication: October 13th, 2008
References and recomended readings (*of special interest, **of outstanding interest)
**1. Alapont JM, Montaner MJ, Pontones JL et al: Carcinoma Prostético de Células Pequeñas. Actas Urológicas Españolas 2002; 26(8):585-88. [ Links ]
**2. Rodríguez Martínez JJ, Herreros Villaraiz M, Pérez Garcia FJ et al. Hemorragia suprarrenal como primera manifestación de un Carcinoma Pulmonar de Células Pequeñas. Arch Esp Urol 2000; 53:726-30. [ Links ]
*3. Lee SS, Lee JL, Ryu MH et al: Extrapulmonary small cell carcinoma: single center experience with 61 patients. Acta Oncol 2007; 46:846-51. [ Links ]
*4. Cicin I, Karagol H, Uzunoglu S et al: Extrapulmonary small-cell carcinoma compared with small-cell lung carcinoma: a retrospective single center study. Cancer 2007; 110:1068-76. [ Links ]
5. Yildirim Y, Akcay Y, Ozyilkan O, Celasun B. Prostate small cell carcinoma and skin metastases: A rare entity. medical principles and practice 2008;17:250-2. [ Links ]
**6. Spiess PE, Pettaway CA, Vakar-Lopez F et al. Treatment outcomes of small cell carcinoma of the prostate. Cancer. 2007;110:1729-37. [ Links ]
7. Yamamoto N, Kinoshita H, Inoue T et al. Small cell carcinoma of the prostate: a case report. Hinyokika Kiyo 2007;53:665-9. [ Links ]

