










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.10 Madrid oct. 2016
PICTURES IN DIGESTIVE PATHOLOGY
Fatal Campylobacter jejuni ileocolitis
Ileocolitis fatal por Campylobacter jejuni
Marta Magaz-Martínez, Aurelio Garrido-Botella, Fernando Pons-Renedo, Borja Oliva-del-Río, Belén Agudo-Castillo, Pilar Ibarrola-Arévalo and Luis Esteban Abreu-García
Department of Gastroenterology. Hospital Puerta de Hierro Majadahonda. Majadahonda, Madrid. Spain
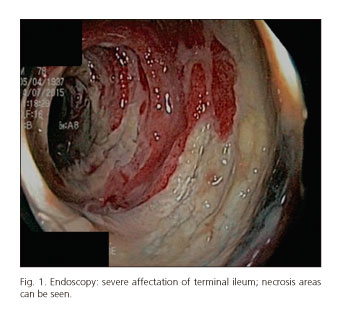
Most Campylobacter infections are mild. We present a case that was fatal. A 78-year-old male was under study due to a three month evolution diarrhea and loss of 7 kg. The colonoscopy requested showed ileo-colonic affection. The ileal mucosa presented intense erythema with edema and large ulcers and necrosis areas. This was the most affected area, as can be seen in the figures, showing a severe and continuous affection (Figs. 1 and 2). The cecum showed loss of vascular pattern and superficial patchy ulcers; from the ascending colon the affection was less severe (Figs. 3 and 4). Multiple serial biopsies were taken. Hospitalization was required. Blood tests highlighted acute renal failure. He received fluid therapy and empirical antibiotics with ciprofloxacin and metronidazole. On the second day, the patient showed abdominal distention, peritonism and hypotension. An emergency CT showed ileitis complicated with intestinal pneumatosis. The patient was moved to ICU, where, after a multiple organ failure with metabolic acidosis, he died within a few hours. Subsequently, both stool cultures and histology revealed infectious active ileocolitis and isolation of macrolide-sensitive and quinolone-resistant Campylobacter jejuni.



Campylobacter infection usually starts in the jejunum and ileum and progresses distally. A differential diagnosis with other infectious colitis (Yersinia, tuberculosis, etc.), ischemic colitis and inflammatory disease should be made. The case fatality rate is low and most occur in elderly or patients with comorbidity as in this case. The mortality rate is estimated at 0.024%.
The treatment is based on proper hydration. Antibiotics should be used in severe cases or in patients at risk (fever, intestinal manifestations, longer than a week infection, immunocompromised or elderly). The choices are macrolides and fluoroquinolones. However, in some countries quinolone resistance is increasing, as in Spain, where the percentage exceeds 50%. We should not forget this fact for the proper treatment approach and specifically in refractory cases.
References
1. Gradel KO, Schønheyder HC, Dethlefsen C, et al. Morbidity and mortality of elderly patients with zoonotic Salmonella and Campylobacter: A population-based study. J Infect 2008;57:214-22. DOI: 10.1016/j.jinf.2008.06.013. [ Links ]
2. Nelson JM, Smith KE, Vugia DJ, et al. Prolonged diarrhea due to ciprofloxacin-resistant campylobacter infection. J Infect Dis 2004;190:1150-7. DOI: 10.1086/423282. [ Links ]
3. Pacanowski J, Lalande V, Lacombe K, et al. CAMPYL Study Group. Campylobacter bacteremia: Clinical features and factors associated with fatal outcome. Clin Infect Dis 2008;47:790-8. DOI: 10.1086/591530. [ Links ]
