










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.20 no.61 Murcia ene. 2021 Epub 01-Feb-2021
https://dx.doi.org/10.6018/eglobal.436421
Originals
Relationship between syphilis cases and family health strategy in northeastern Brazil
1Complex of Medical Sciences and Nursing - CMSN, Federal University of Alagoas / Campus Arapiraca, Brazil.
Objectives:
This study aims to verify the relationships between the advancing of coverage of the Family Health Strategy in the nine northeastern states and the rates of detection of syphilis in pregnant women and congenital between the years 2008 and 2017.
Methods:
Observational, descriptive and cross-sectional study, in which the detection rates for gestational syphilis and congenital in the nine states of the Northeast and this region as a whole were correlated with the respective annual averages Family Health Strategy coverage. For that, Pearson's correlation coefficient test was performed for these two variables, using the Statistical Package for the Social Sciences 25 software.
Results:
The statistical analysis of the state data made it possible to identify that, as well as in the grouped data of the region, as the Family Health Strategy coverage increased, the detection rate of syphilis cases in pregnant women and congenital also increased significantly in most states, and in the Northeast region entirely.
Conclusions:
The Unified Health System through the Family Health Strategy has made great advances related to the monitoring of pregnancy, puerperium and child development as in the early diagnosis of infections like syphilis. However, in addition to the diagnosis, significant improvements are needed in the treatment and prevention of these diseases in the Northeast region.
Keywords: Syphilis; Prenatal Care; Family Health Strategy
INTRODUCTION
Health is recognized by the Brazilian Federal Constitution of 1988 as an everybody's right and obligation of the State 1. In the effectuation of this right, the Primary Care in Health (PCH) has an important role, offering more than the assistance services, actions of promotion and prevention, looking to guarantee the universal access to health 2. In the 90`s decade, with the implantation of the Unified Health Service (UHS) and, mainly, with the Family Health Strategy (FHS) in 2006, a new paradigm in the health politics of Brazil began, through the integral and continuous attention focusing on the family 3.
The FHS, through your highlight in relation to the integrality, has impacted in the health conditions of the people, especially in the poorer areas. Because of your efficacy and importance in the Brazilian social panorama, the FHS expanded and is structuring the PCH, guaranteeing a reduction in the hospitalization, malnutrition and child mortality, through the expansion of vaccinal programs and the ampliation of the gateway of the Unified Health Service (UHS), through changes in the assistance model 4.
Among the developed actions by the FHS, the health education, the monitoring of the pregnancy, the puerperium, the firsts months of life of the newborn, as well as of the child development are key components for a proper assistance for the people 5. In this sense, the prevention and the treatment of the sexually transmitted infections (STIs) deserve a spotlight, not only in the prenatal, as also in the puerperal and neonatal periods, given that the possibility of vertical transmission of some of these infections, as the monitoring of the partners and the general population 6.
In this context, the syphilis deserves a spotlight because of the national raise of the amount of cases in the last years, both in pregnant women and in the congenital form 7. Its clinical manifestations result from the infection by the spirochete bacteria Treponema pallidum, that is acquired, mainly, sexually or vertically. When the transplacental transmission occurs, there is a possibility of prematurity, abortion or fetal death, beside the sequels, like deafness, learning difficulty, progression of damages of the teeth, eyes and joints, which are frequently irreversible 8.
Among other grievances, the congenital syphilis (CS) is inside the evitable perinatal causes, through effectives diagnosis and treatment during the pregnancy. Therefore, there is a direct relationship between its control and the quality of the prenatal assistance, justifying the need of monitoring, valuation and improvement of this action in the different services and levels of complexity 9. Hereupon, an adequate FHS coverage is indispensable for a better prenatal assistance that, consequently, will impact in the gestational (GS) and congenital syphilis 10.
Considering the importance of the FHS in the PCH`s structuration and in the quality of the health access of the population, its impact is noticeable, especially in regions with big social vulnerability, like in the Northeast, a Brazilian region historically marked per great socioeconomic differences 11. This study aims to know the relationships that exist between the progress in the coverage of the Family Health Strategy in the nine states of the Brazilian Northeast and the gestational and congenital syphilis detection rates between the years of 2008 and 2017.
MATERIAL AND METHOD
This is an observational, descriptive and transversal study, in which the relationship between the FHS coverage and the number of cases of GS and CS was analyzed. The detection rates of both diseases in the nine states of the Northeast region, as well as of the entire region, between the years of 2008 and 2017, from information obtained on the website of the Chronic Conditions and Sexually Transmitted Infections Department (CCSTID) from the Health Ministry (HS), were used to determine the study population.
The information about the FHS coverage was cataloged through the database of the Primary Care of Health Secretary (PCHS) from the HS. Subsequently, the average coverage was calculated for each of the years of the study, for each of the states and for the entire region.
The data were also cross-checked, correlating the detection rates for GS and CS from all the nine states of Northeast and from this region as a whole with their respective FHS annual coverage averages. For this, Pearson's correlation coefficient test was performed for these two variables, using the Statistical Package for the Social Sciences 25 (SPSS) software.
The SPSS is a program and a statistical package with different modules, embracive and easy to handle, developed by IBM. Its main functions are data preparation and validation, regression models, advanced statistical models, tables, trends, categories, geospatial analysis and simulation functions. Pearson's exact test or chi-square test, in turn, is used when it is desired to analyze the association between a nominal variable and another nominal or ordinal variable, being liable to be calculated by the aforementioned program.
A significance level of <0.05% was assumed for these analyzes. The data were organized and stored by the Microsoft Office Excel program (version 2013), and analyzed by SPSS (version 25.0), considering r ≥ 0.100 (there is no significant correlation between the variables); 0.050 ≤ r <0.100 (there is a weak correlation between the variables); 0.010 ≤ r <0.050 (there is a significant correlation between the variables); 0.001 ≤ r <0.010 (there is a highly significant correlation between the variables); p <0.001 (there is an extremely significant correlation between the variables).
For using only secondary and publicly available data, the appreciation from the Human Research Ethics Committee was waived, according to the Resolutions 466/12, 510/16 and 580/18 from the Health National Council of Brazil.
RESULTS
In the analyzed time interval, an increase of the detection rate of syphilis cases during pregnancy (435%) was identified, as well as cases of congenital syphilis (285%) in the Northeast. The year of 2017 is worth mentioning, in which about 66.000 live births (LB) were affected by the congenital form of this disease (8.1 cases per 1.000 LB). At the same time, there was an increase of 11.6% in the FHS coverage, (average of 79.15% in the period) (Table 1). The statistical treatment utilized showed that the expansion of this strategy, between 2008 and 2017, has an extremely significant correlation with the increase in the detection rate of GS (r=0.000) and CS (r=0.000) (Table 1, Figures 1 and 2).
Table 1. Detection rates of syphilis in pregnant women and congenital syphilis per year of diagnosis and FHS coverage, Northeast region, Brazil, 2008-2017
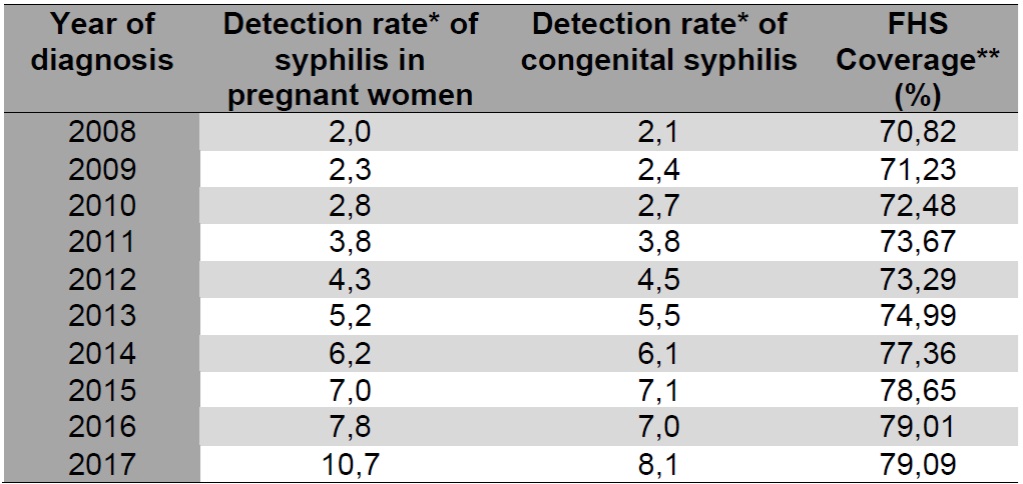
Source: CCSTID/PCHS
*Cases per 1.000 newborns per year of diagnosis
**Average annual coverage

Source: authors
Figure 1. Simple scatterplot showing the correlation between the FHS coverage (%) and syphilis rate in pregnancy per one thousand live births with an adjustment line, Northeast, Brazil, 2008-2017.

Source: authors
Figure 2. Simple scatterplot showing the correlation between the FHS coverage (%) and congenital syphilis rate per one thousand live births with an adjustment line, Northeast, Brazil, 2008-2017.
The statistical analysis of the data from the states made it possible to identify that, like in the grouped data of the region, as the FHS coverage increased, the detection rate of cases of GS also increased significantly in most states. However, of the nine states of Northeast, in only one, Paraíba, this association was negative, showing an increase in FHS coverage, however with a reduction in the detection rate. The states Rio Grande do Norte and Sergipe also showed different behavior, since no correlation was observed between the variables through the model adopted for analysis. Among the analyzed states, the one that showed the greatest positive association was Bahia (Table 2).
Table 2. Correlation between the FHS coverage and the detection rate of syphilis in pregnant women, Northeast, Brazil, 2008-2017.

Sources: Authors
In relation to CS, the correlations were very similar to what was seen with GS, meaning that there was a correlation between the expansion of the FHS coverage and the increase in the CS detection rate in most states, with emphasis on Bahia and Pernambuco, where this correlation was stronger. Unlike most states, Rio Grande do Norte, Sergipe and Paraíba did not show an association between the variables (Table 3).

DISCUSSION
The incidence rates of CS and GS are known as sentinels of the health service, because they reveal information about the assistance provided, mainly to the pregnant woman and the newborn. As it is a preventable and treatable disease, the sustenance of high rates may suggest vulnerabilities in the health service 12, which allow both the emergence of new cases and high levels of underreporting of the disease 13.
This study identified an increase in the FHS coverage, followed by higher rates of detection of CS and GS in most states of the Northeast region, with the exception of the states Paraíba, Sergipe and Rio Grande do Norte, that did not show a positive correlation between the FHS coverage and the notification of cases of GS and CS in the adopted analysis method, a phenomenon that can be explained by underreporting 14 and by the reduction of public health investments experienced mainly after a period of financial crisis in Brazil, between 2014 and 2017, which culminated in great political instability and freezing of health spending and investments 15.
The positive correlations between the FHS coverage and the detection of CS and GS identified in this analysis corroborate with other studies, such as a similar one carried out in the state of Goiás 10. This finding suggests a causal relationship of these factors with the expansion of Primary Care in Brazil, which, through the FHS, promoted an improvement in the quality of the prenatal and newborn care, which have, in their protocols, the screening and notification of syphilis in both the pregnant woman and the child who was exposed to the bacteria, thus reducing underreporting, with emphasis from 2017, through the adoption of broader criteria in the definition of cases of GS and CS, contributing to the improvement of the reliability of the most recent data13.
Studies also affirm that the expansion of testing in primary care - the FHS's field of action - provided an increased ability to identify asymptomatic people with syphilis, resulting in the increase of cases of acquired syphilis, GS and CS. They also claim that the teams that performed rapid tests significantly expanded the identification and notification of cases in pregnant women, enabling rapid and timely prenatal care and treatment, even in asymptomatic cases, thus reducing the possibility of fetal infection16.
Another aspect that suggests the causal relationship is the implantation and expansion of the Cegonha Network, since 2011, establishing guidelines for quality maternal and child care and reinforcing the monitoring of the pregnancy jointly with the PHC, especially in cases with higher risk 17. The influence of this strategy in detecting these diseases was also pointed out in a study based on data from Maranhão 18.
However, other factors must be considered in the analysis of the increase of the detection rate of GS and CS in the studied period, including the expansion of STIs 19. The greater occurrence of acquired syphilis in the studied states suggests an increase of unprotected sexual practices, impacting the growth of cases of GS and reflecting on the difficulty of interrupting the syphilis transmission chain, mainly due to the reinfection of pregnant women through untreated sexual partnerships 13.
Furthermore, researches 12,20 show difficulties, such as insufficient knowledge and technical qualification of health professionals to face the problem of syphilis in prenatal care. Another important factor was the shortage of national penicillin, mainly in 2015 21, which can explain the higher GS and CS rates in the Northeast in 2017.
Other studies also relate such growth to the socioeconomic conditions of the population, meaning that many aspects would be interacting for this increase of cases and not only the increase of notifications. Elements such as the population profile, social vulnerability and weaknesses found in the health system and in the access to it by the poorest population can be related to the maintenance of high rates of CS 22. This hypothesis is supported by observing the population profile most affected by the disease, which is more prevalent in black women, with low education level, low socioeconomic status and worse access to health services, making them more vulnerable to the syphilis infection and other diseases, in addition to reducing the access to appropriate treatment 23,24.
Even in the face of these vulnerabilities, the Unified Health System, mainly through the FHS, has made major advances related to the monitoring of the pregnancy, puerperium and child development, resulting in a better quality of life for the population and in family planning, as it democratizes the access to health and allows the work to be adapted to the reality of the assisted community.
Finally, it is emphasized that the study on screen has limitations, as it involves the analysis of secondary data from the Health Information Systems, it may present flaws in the notification of cases. Nevertheless, it is believed that, as these are official data and must be completed in all health services, even if such flaws are considered, they do not annul the results achieved and their results allowed the achievement of the proposed objectives.
CONCLUSIONS
Therefore, it was found through the statistical model used, that the expansion of the Family Health Strategy, between 2008 and 2017, had a positive and significant correlation with an increase of the detection rate of Syphilis in Pregnant Women and of Congenital Syphilis in the following states of Northeast: Alagoas, Bahia, Ceará, Maranhão, Pernambuco and Piauí. No significant relationship was found between the detection rate of CS and the FHS coverage in Sergipe, Rio Grande do Norte and Paraíba. There is also no correlation between the GS detection rate and the FHS coverage in Sergipe and Rio Grande do Norte, but in Paraíba, an inversely proportional relationship between these two variables was found.
Even in the face of these vulnerabilities, the Unified Health System, mainly through the FHS, has made major advances related to the monitoring of the pregnancy, puerperium and child development, resulting in a better quality of life for the population and in family planning, as it democratizes the access to health and allows the work to be adapted to the reality of the assisted community.
However, despite efforts to increase the FHS coverage and reduce the rates of syphilis infections, the Northeast presents major challenges, given that its numbers remain beyond what is desired. This scenario is influenced by several aspects that perpetuate not only the maintenance of high syphilis rates, but also of other STIs and encompass from social weaknesses to problems related to the management of resources invested in health and the lack of investments in continuing professional education, making the management of these diseases difficult.
REFERENCIAS
1. Brasil. Senado Federal. Constituição da República Federativa do Brasil. Texto constitucional promulgado em 5 de outubro de 1988, com as alterações determinadas pelas Emendas Constitucionais de Revisão nos 1 a 6/94, pelas Emendas Constitucionais nos 1/92 a 91/2016 e pelo Decreto Legislativo no 186/2008. Brasília (DF); 1988. [acesso em 18 de janeiro de 2020]. Disponível em: https://www2.senado.leg.br/bdsf/bitstream/handle/id/518231/CF88_Livro_EC91_2016.pdf [ Links ]
2. Guerra M. Modelo de alocação de recursos do sistema único de saúde para organizações hospitalares: serviços de alta complexidade. [tese]. Brasília: Universidade de Brasília. 2013. [ Links ]
3. Castro ALB. Atenção Primária e relações público privadas no Sistema de Saúde do Brasil [tese]. Rio de Janeiro: Escola Nacional de Saúde Pública Sergio Arouca, Fundação Oswaldo Cruz, 2015. [ Links ]
4. Neves RG, Flores TR, Duro SMS, Nunes BP, Tomasi E. Tendência temporal da cobertura da Estratégia Saúde da Família no Brasil, regiões e Unidades da Federação, 2006-2016. Epidemiol Serv Saude. [periódico on-line]. 2018. [Acesso em 11 de maio de 2020]. 27(3):e2017170. Disponível em: https://www.scielo.br/scielo.php?script=sci_abstract&pid=S2237-96222018000300302&lng=pt&nrm=iso&tlng=pt [ Links ]
5. Arantes LJ, Shimizu HE, Hamann EM. Contribuições e desafios da Estratégia Saúde da Família na Atenção Primária à Saúde no Brasil: revisão da literatura. Ciênc saúde coletiva [periódico on-line]. Maio de 2016 [acesso em 18 de janeiro de 2020]; 21(5): 1499-1510. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232016000501499&lng=en [ Links ]
6. Brasil. Ministério da Saúde. Portaria MS/GM no 1.459, de 24 de julho de 2011. Institui, no âmbito do Sistema Único de Saúde - SUS - a Rede Cegonha. Brasília (DF), 2011. [acesso em 18 de janeiro de 2020]. Disponível em: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt1459_24_06_2011.html [ Links ]
7. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Boletim epidemiológico sífilis 2018. Brasília (DF); outubro de 2018; volume 49, nº 45. [acesso em 18 de janeiro de 2020]. Disponível em: http://www.aids.gov.br/pt-br/pub/2018/boletim-epidemiologico-de-sifilis-2018 [ Links ]
8. Andrade HS, Rezende NFG, Gacia MN, Guimarães EAA. Caracterização epidemiológica dos casos de sífilis em mulheres. Ciência & Saúde [periódico on-line]. 2019 [acesso em 18 de janeiro de 2020]. Disponível em: http://revistaseletronicas.pucrs.br/ojs/index.php/faenfi/article/view/32124/17807 [ Links ]
9. Cardoso ARP, Araújo MAL, Cavalcante MS, Frota MA, Melo SP. Análise dos casos de sífilis gestacional e congênita nos anos de 2008 a 2010 em Fortaleza, Ceará, Brasil. Ciênc saúde coletiva [periódico on-line]. Fevereiro de 2018 [Acesso em 11 de março de 2020]; 23( 2 ): 563-574. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232018000200563&lng=en [ Links ]
10. Nunes PS, Zara ALSA, Rocha DFNC, Marinho TA, Mandacarú PMP, Turchi MD. Sífilis gestacional e congênita e sua relação com a cobertura da Estratégia Saúde da Família, Goiás, 2007-2014: um estudo ecológico. Epidemiol Serv Saude. [periódico on-line]. 2018. [Acesso em 11 de maio de 2020]. 27(4):e2018127. Disponível em: https://www.scielo.br/scielo.php?script=sci_abstract&pid=S2237-96222018000400313&lng=pt&nrm=iso [ Links ]
11. Carvalho FC, Vasconcelos TB, Arruda GMMS, Macena RHM. Modificações nos indicadores sociais na região Nordeste após a implementação da Atenção Primária. Trab Educ Saúde [periódico on-line]. 2019 [Acesso em 11 de março de 2020]. Disponível em: https://www.scielo.br/scielo.php?script=sci_arttext&pid=S1981-77462019000200503 [ Links ]
12. Domingues RMSM, Saracen V, Hartz ZMA, Leal MC. Sífilis congênita: evento sentinela da qualidade da assistência pré-natal. Rev Saúde Pública. [periódico on-line]. 2013. [Acesso em 11 de maio de 2020]. 47(1): 147-157. Disponível em: https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102013000100019 [ Links ]
13. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Boletim Epidemiológico Sífilis 2017. Brasília (DF); 2017; volume 48, nº 36. [acesso em 18 de janeiro de 2020]. Disponível em: http://www.aids.gov.br/pt-br/pub/2017/boletim-epidemiologico-de-sifilis-2017 [ Links ]
14. Lafetá KRG, Martelli Júnior H, Silveira MF, Parnaíba LMR. Sífilis materna e congênita, subnotificação e difícil controle. Rev Bras Epidemiol [periódico on-line]. 2016. [Acesso em 11 de maio de 2020]. 19 (1): 63-74. Disponível em: https://www.scielo.br/scielo.php?pid=S1415-790X2016000100063&script=sci_abstract&tlng=pt [ Links ]
15. Melo EA, De mendonça MHM, Teixeira M. A crise econômica e a Atenção Primária à Saúde da cidade do Rio de Janeiro, Brasil. Ciência & Saúde Coletiva. [periódico on-line]. 2019. [Acesso em 11 de maio de 2020]. 24(12):4593-4598. Disponível em: https://www.scielo.br/scielo.php?pid=S1413-81232019001204593&script=sci_arttext [ Links ]
16. Figueiredo DCMM, Figueiredo AM, Souza TKB, Tavares G, Vianna RPT. Relação entre oferta de diagnóstico e tratamento da sífilis na atenção básica sobre a incidência de sífilis gestacional e congênita. Cad Saúde Pública. [periódico on-line]. 2020. [Acesso em 05 de maio de 2020]. 36 (3):e00074519. Disponível em: https://www.scielo.br/scielo.php?pid=S0102-311X2020000305009&script=sci_arttext [ Links ]
17. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Implantação das Redes de Atenção à Saúde e Outras Estratégias da SAS. Brasília (DF); 2014. [acesso em 18 de janeiro de 2020]. Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/implantacao_redes_atencao_saude_sas.pdf [ Links ]
18. Moraes BQS, Machado MF, Sousa CDF. Impacto da rede cegonha nas tendências de sífilis no Maranhão 2008-2017. UNITPAC. [periódico on-line]. 2020. [Acesso em 05 de maio de 2020]. 13 (1): 64-71. Disponível em: https://www.researchgate.net/publication/340237750_IMPACTO_DA_REDE_CEGONHA_NAS_TENDENCIAS_DE_SIFILIS_NO_MARANHAO_2008-2017 [ Links ]
19. Kenyon C, Buyze J, Colebunders R. Classification of incidence and prevalence of certain sexually transmitted infections by world regions. Int JInfect Dis. [periódico on-line]. 2014. [Acesso em 11 de maio de 2020]. 18: 73-80. Disponível em: https://www.ijidonline.com/article/S1201-9712(13)00306-8/fulltext [ Links ]
20. Lazarini FM, Barbosa DA. Intervenção educacional na atenção básica para prevenção da sífilis congênita. Rev Latino-Am Enfermagem. [periódico on-line]. 2017. [Acesso em 11 de maio de 2020]. 25:e2845. Disponível em: https://www.scielo.br/pdf/rlae/v25/pt_0104-1169-rlae-25-02845.pdf [ Links ]
21. Brasil. Ministério da Saúde. Nota Informativa Conjunta Nº 109/2015/GAB/SCTIE/MS. Orienta a respeito da priorização da penicilina G benzatina para sífilis em gestantes e penicilina cristalina para sífilis congênita no país e alternativas para o tratamento da sífilis. Brasília (DF); 2015. [acesso em 18 de janeiro de 2020]. Disponível em: http://www.aids.gov.br/pt-br/legislacao/nota-informativa-conjunta-no-109105gabsvsms-gabsctiems [ Links ]
22. Araújo CL, Shimizu HE, Sousa AIA, Hamann EM. Incidência da sífilis congênita no Brasil e sua relação com a Estratégia Saúde da Família. Rev Saúde Pública [periódico on-line]. Junho de 2012 [acesso em 18 de janeiro de 2020]; 46(3): 479-486. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102012000300010&lng=en [ Links ]
23. Cavalcante PAM, Pereira RBL, Castro JGD. Sífilis gestacional e congênita em Palmas, Tocantins, 2007-2014. Epidemiol Serv Saúde [periódico on-line]. Junho de 2017 [Acesso em 11 de março de 2020]; 26(2): 255-264. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S2237-96222017000200255&lng=pt https://doi.org/10.5123/s1679-49742017000200003 [ Links ]
24. Leal MC, Gama SGN, Pereira APE, Pacheco VE, Carmo CN, Santos RV. A cor da dor: iniquidades raciais na atenção pré-natal e ao parto no Brasil. Cad Saúde Pública. [periódico on-line]. 2017. [Acesso em 11 de maio de 2020]. 33 (Sup 1):e00078816. Disponível em: https://www.scielo.br/pdf/csp/v33s1/1678-4464-csp-33-s1-e00078816.pdf [ Links ]
Received: July 09, 2020; Accepted: September 07, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
