










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versão On-line ISSN 2173-2345versão impressa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.14 no.2 Madrid Abr./Jun. 2022 Epub 12-Set-2022
https://dx.doi.org/10.4321/s1889-836x2022000200006
ORIGINALS
Description of the patients treated at the Fracture and Fall Prevention Unit in the context of a Fracture Liaison Service. FLS Anoia
1Physiotherapy Service. Social Health Foundation Sant Josep de Igualada. Barcelona (Spain)
2Acute Geriatric Unit. Geriatric Service. University Hospital of Igualada. Barcelona (Spain)
3Occupational Therapy Service. Fundación Sanitaria Sant Josep de Igualada. Barcelona (Spain)
Objective:
The aim of this study is to present the performance, treatment and functional results obtained in a Fracture and Fall Prevention Unit.
Methods:
Descriptive prospective study of patients with previous osteoporotic fracture, treated between April 25, 2016 and November 20, 2017.
Results:
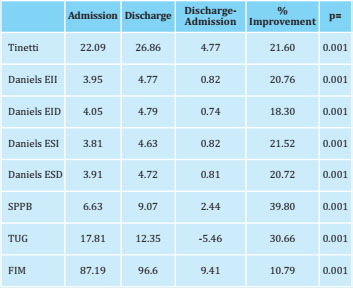
We analyzed 43 patients with a mean age of 80.2 years (SD±5.19), 81.40% women (n=35). Number of fractures 61,28% hip (n=17), 25% vertebral (n=15) and 21% distal radius (n=13). At discharge, all the assessment scales used improved, highlighting the results of the SPPB (39.80%), TUG (30.66%) and Tinetti (21.60%).
Conclusions:
The profile patient treated corresponds to an 80.2-year-old woman, with a hip fracture, Tinetti 22:09, Daniels in extremities of 3.95, 4:05, 3.81, 3.91, SPPB of 6.63, TUG of 17.81 and FIM of 87.19 points. An improved score in all the assessed scales is reported.
Key words Fall prevention unit; elderly; fragility fracture; Fracture Liaison Service
INTRODUCTION
Worldwide, 1 in 3 women and 1 in 5 men will experience a fragility fracture in their lifetime. Every 3 seconds there is 1 fragility fracture in the world. The most frequent fractures associated with osteoporosis are located in the hip, spine and wrist1,2.
Hip fracture has become an international barometer of osteoporosis, associated with low bone mineral density, high health care costs, and greater disability than other types of osteoporotic fracture3. Only 30% of people with a hip fracture regain their pre-fracture level of physical function, and many are left with reduced mobility, loss of functional independence, and requiring long-term care. For this reason, among other reasons, the International Osteoporosis Foundation (IOF) has developed the Capture the Fracture program, aimed at reducing secondary and posterior fractures by facilitating the implementation of Fracture Liaison Services (FLS)1, 2.
The IOF Best Practice Framework (BPF) is an internationally recognized clinical guideline for the secondary prevention of osteoporotic fractures. Structured in a series of 13 standards, the BPF addresses key elements for the success of the FLS and also includes suitability objectives, thereby stimulating excellence. Specifically, in standard number 7, fall prevention is mentioned as one of the key elements1,2. This led us to found a Fall Prevention Unit which we named the School of Secondary Prevention of Fractures and Falls (EPFiC, based on the Spanish title) of the Sant Josep Health Foundation (FSSJ) within the framework of the FLS Anoia.
When we focus on frailty models, such as Fried's or Watson's, many of the risk factors associated with falls are included, such as: muscle weakness, weight loss, balance disturbances, decreased gait speed, fatigue, low level of physical activity and cognitive impairment5.
Frailty, expressed as vulnerability to adverse events, explains loss of functional capacity, falls, disability, and dependency. Between 25-28% of 80-year-olds are frail, and there is a direct relationship between frailty and falls, these being the leading cause of mortality in the elderly6. In addition, falls generate fear of falling and this reduces physical functioning, social activities, loss of confidence, dependency, social isolation and decreased quality of life4. We therefore refer to the deterioration of physical performance and falls are among the most robust factors that tend to activate the negative spiral of frailty5.
The only interventions that have been shown to be effective in preventing, and even reversing, the state of frailty in elderly patients are physical exercise, comprehensive geriatric assessment and management of the main geriatric syndromes, ahead of nutritional interventions or the use of certain drugs7.
Having a good state of health and functionality are predictors of residing at home and maintaining functionality prior to a year after a hip fracture, while the worst state of health and functionality are predictors of mortality8-10.
It is worth noting, therefore, the importance of the implementation of Fall Prevention Units, such as the School for the Prevention of Fractures and Falls (EPFiC) of the FSSJ, which began its activity in April 2016 within the framework of the FLS Anoia, in which They can provide a reduction in the risk of falls between 30% and 50%. It is reported that 50% of falls are due to multiple factors. The most prevalent associated factors are orthostatic hypotension, chronic arthropathy pain and vestibular syndrome11.
Carrying out preventive actions to keep our elderly population out of risk and maintain a good level of functionality are essential EPFiC objectives. One of our maxims as health professionals should be to empower our society to guarantee active aging.
Unlike the proposed functional plan of the Fall Prevention Units of the Spanish Society of Geriatrics and Gerontology12, our EPFiC's target population encompasses those patients with a previous fracture, since it is this group that benefits most by reducing the risk of new fractures when starting an anti-osteoporotic pharmacological treatment2.
Here we describe the School of Secondary Prevention of Fractures and Falls (EPFiC) care protocol and show the functional results obtained in the first 19 months after its implementation.
MATERIAL AND METHODS
Description of the EPFiC care protocol
Patients with fractures due to bone fragility are recruited at the Social Health Center of the FSSJ, by telephone, after receiving the request for assessment through 3 recruitment routes: from 1. Outpatient Consultations of the Hospital of Igualada: a) Geriatrics (Consultation for fractures due to bone fragility), b) Rheumatology and c) Physical Medicine; 2. Primary Care and 3. Socio-Health Care. The inclusion and exclusion criteria agreed upon in the FLS Anoia are followed and are shown in figure 1.
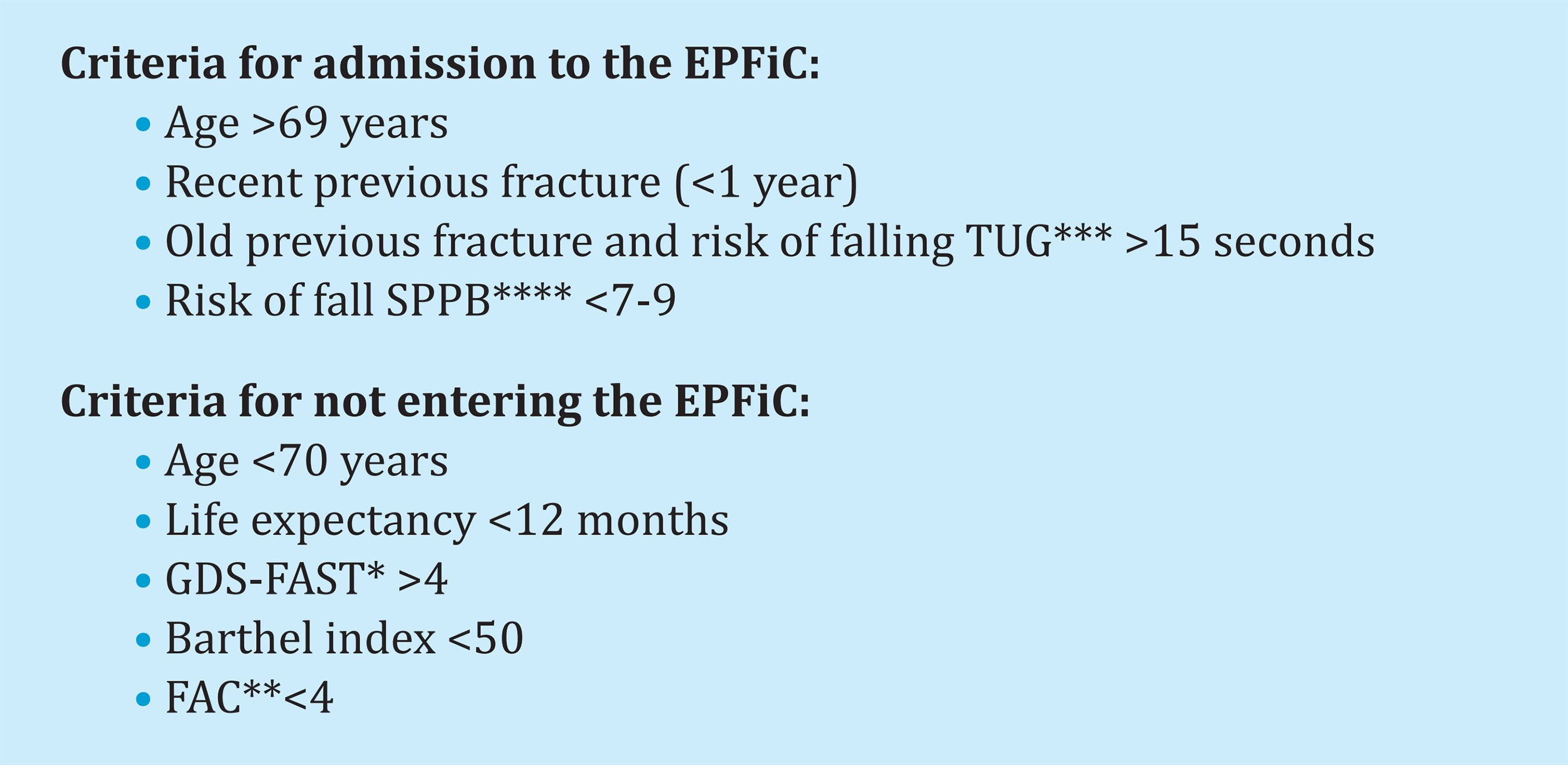
*GDS‐FAST: Geriatric Dementia Scale. **FAC: Functional Ambulation Classification. ***TUG: Time Up and Go. ****SPPB: Short Physical Performance Battery.
Figure 1. EPFiC admission/non-admission criteria for the FSSJ
They are scheduled for initial functional assessment of occupational therapy and physiotherapy, with nursing supervision and support from the FFSJ rehabilitation day hospital. In this functional assessment, our staff recorded Tinetti and Daniels balance scale values for muscle strength, the Timed Up and Go (TUG) for the risk of falls, the Short Physical Performance Battery (SPPB) for frailty and Functional Independence Measure (FIM) for functional independence.
After this first assessment, the patient will carry out 24 group sessions, with a maximum of 8 people, 3 days a week on alternate days and lasting 1.45 hours. The main therapeutic components are balance re-education, strength re-training, active mobility, proprioception, vestibular re-education and re-education of the motor sequence to get up after a fall, as well as ADLs and IADLs. This therapeutic prescription schedule is coupled with exercise recommendations to improve balance and strength explained in the PreFIT Clinical Trial protocol13,14 and in the systematic review by Sherrington C, et al.15, as essential elements in exercise programs to prevents falls.
In addition, the patient receives an informative and educational class on nutrition and healthy habits by the dietician-nutritionist of the FSSJ for 1.5 hours, having completed the 24 group sessions. Finally, all the functional assessment scales are reassessed before discharge, and they respond to a satisfaction questionnaire.
Study design and participants
This is a prospective descriptive study of patients treated at the EPFiC in the period between April 25, 2016 and November 20, 2017.
Variables
For the analysis of the data obtained, pre-post intervention, socio-demographic variables have been collected: age, sex and type of fracture; Functional assessment variables: Tinetti scale, Daniels (right (R) and left (L) of upper limbs (UL) and lower extremities (LE)), Timed Up and Go (TUG), Short Physical Performance Battery (SPPB) and the Functional Independence Measure (FIM).
The data obtained from the satisfaction questionnaire is obtained through an unvalidated questionnaire for internal use.
This study has been approved by the Hospital de Bellvitge Ethics Committee.(PR222/15).
Statistics
In the description of the cohort, percentages and frequencies have been used for qualitative variables and medians and standard deviations for quantitative variables. To study the relationship between categorical variables, the Chi square test was used, with the correlation of Fisher's exact test for the comparison of proportions, depending on the frequencies. P-values less than or equal to 0.05 were considered statistically significant. The statistical program SPSS version 19.0 (IBM Corporation, Chicago Illinois) was used.
RESULTS
During the study period, 45 patients were treated, 2 of whom did not complete the study, leaving a total sample of 43 patients with a mean age of 80.2 years (SD±5.19), 81.40% being women (n=35).
Number of fractures 61, of which 28% were of the hip (n=17), 25% vertebral (n=15), 21% Colles-Distal radius (n=13), 8% humerus (n=5), 5% pelvis (n=3), 5% ribs (n=3), 2% femur (n=1) and 6% other fractures (n=4).
At the time of discharge, an improvement is shown in all the assessment scales used, highlighting the improvement in the SPPB of 39.80%, of the TUG in 30.66% and in the Tinetti balance scale of 21.60% (table 1).
The satisfaction surveys collected were 36 of the 43 patients recruited, representing 83.7% participation. Of these, the average satisfaction score of the EPFiC is 9.7 points out of a maximum of 10. The 7 patients for whom there is no record of the survey was due to the fact that they did not submit it at the time of discharge.
DISCUSSION
In terms of methodology, our study coincides with the Clinical Trial Prefit14 in the recruitment of patients who are in the community and who are older than 70 years.
The functional recovery obtained reflected in the improvement in the score of the scales used, especially the Tinetti scale with 21.60%, the SPPB with 39.60% and the TUG with 30.66%, cannot be correlated with a decrease in the number of falls, nor in the reduction in the number of fractures due to the design of our descriptive study. To a certain extent, the score improvement of these 3 scales could lead us to believe that the risk of falls will be reduced. This is implied by the very definition of each of the three scales in which, the better the result, the lower the risk of falls. As pointed out in the systematic review by Sherrington et al.15, with a high level of evidence, exercise programs that include balance, functional and resistance exercises reduce the rate of falls and the number of people who experience falls, in people older people living in the community. Zhao et al.16 also concluded that exercise had a beneficial effect in reducing fall-related fractures and reduces risk factors for fall-related fractures in older people. Hopewell et al.17 conclude their metaanalysis by saying that, of all the multi-factor interventions, exercise prescription can reduce the rate of falls and slightly reduce the risk of one or more falls and recurrent falls in older people throughout the community.
Most of the people we have assessed with fractures due to bone fragility are women, 81.40% of the sample. The results by gender expressed by Roca F et al.11 were also women who predominated, but in reference to falls, without being able to confirm if they were also the ones who had a higher incidence of fractures. In any case, knowing that a TUG greater than 15 seconds correlates with the risk of falling and if we look at the average TUG on admission, we can mention that there is a risk of falls and possible fractures that is reduced at the time of discharge as as reflected by the reduction of 5.46 seconds of the TUG.
In our study, the most prevalent fractures were hip in 28%, vertebra in 25% and distal radius in 21%. Currently we have not found studies of fall prevention units that provide data that allow us to compare in this regard. We have already commented recently that the great challenge of the 21st century should be the creation of multiprofessional osteoporotic fracture units in an effort to reduce the incidence of major fractures due to bone fragility (vertebra, pelvis, hip and humerus) and especially hip fractures18.
Thus, we believe that we must redirect our efforts towards post-fracture secondary prevention, in its double version of treating osteoporosis and falls, in those people who have already had a fracture due to bone fragility.
In contrast to the proposed functional plan of a Unit for the Falls Prevention and Osteoporotic Fractures of the Spanish Society of Geriatrics and Gerontology12 who recommend working with the elderly person who was at risk of falling or who had already fallen as a result of an osteoporotic fracture or not, our study, we focus on working with people who, although they may be at risk of falling, or have suffered previous falls, must all have a history of fracture due to bone fragility. We have considered this modification, following the recommendations of the IOF Capture the Fracture program, in which it is this population group, with a previous osteoporotic fracture, who benefits most from pharmacological intervention. Along these lines, we believe that it is this population that could benefit most from fracture and fall prevention units, bearing in mind that studies with a robust design and methodology are required to demonstrate this.
As a multidisciplinary and multilevel group, within the framework of the FLS, our aim was to implement a fracture and fall prevention unit in the context of secondary prevention in osteoporotic fractures or due to bone fragility. We are aware of the difficulties involved in organizing referral circuits and recruiting patients, given FLS Anoia's different health institutions.
Last but not least, the participants' degree of satisfaction is noteworthy, with an average score of 9.7 points out of 10. This was one of the crucial aspects for adherence during the intervention.
Based on our experience, we would encourage EPFiC implementation in the public health system, as well as city council strategic community health plans to guarantee adherence to therapeutic physical activity that the EPFiC has already begun. Without a doubt, this needs continuity in the community.
LIMITATIONS
As this is a descriptive study, we cannot correlate the findings of functional improvement with a decrease, or not, in falls or new fractures in this target population. Furthermore, the satisfaction questionnaire is for internal use and not validated. However, these limitations are elements for improvement in future research studies already under way.
CONCLUSIONS
Based on our findings, the profile of the post-fracture patient due to bone fragility treated at the EPFiC of the San José Health Foundation (FSSJ) in Igualada, is an 80.2-yearold woman with a hip fracture, Tinetti 22.09, Daniels in LLL, RLL, LUL and RUL of 3.95, 4:05, 3.81, 3.91 respectively, SPPB of 6.63, TUG of 17.81 and FIM of 87.19 points.
At the time of discharge, after the 24-session group treatment, a statistically significant improvement was observed in the scores of all the assessed scales. This would correlate with a reduced risk of falling. However, we do not know if this correlates with a reduction in the number of falls and, specifically, with a reduction in the number of new fractures due to bone fragility. Future studies with a very robust methodology are required.
Bibliografía
1 Akesson K, Marsh D, Mitchell PJ, McLellan AR, Stenmark J, Pierroz DD, Kyer C, Cooper C; IOF Fracture Working Group (2013) Capture the Fracture: a Best Practice Framework and global campaign to break the fragility fracture cycle. Osteoporos Int. 24:2135-2152. [ Links ]
2 www.capturethefracture.org. [ Links ]
3 Zidén L. Life after hip fracture.Impact of home rehabilitation versus conventional care and patients' experiences of the recovery process in a short-and long-term perspective. Institute of Neuroscience and Physiology at Sahlgrenska Academy. University of Gothenburg. 2008. [ Links ]
4 Diong J, Allen N, Sherrington C. Structured exercise improves mobility after hip fracture: a meta-analysis with meta-regression. Br J Sports Med. 2015;0:1-11. [ Links ]
5 Zidén L, Häggblom-Kronlöf G, Gustafsson S, Lundin-Olsson L, Dahlin-Ivanoff. Physical Function and Fear of Falling 2 Years After the Health-Promoting Randomized Controlled Trial: Elderly Persons in the Risk Zone. The Gerontologist 2013; Vol. 54, No. 3, 387-397. doi:10.1093/geront/gnt078. [ Links ]
6 Lopez P, Izquierdo M, Radaelli R, Sbruzzi G, Grazioli R, Pinto RS, Cadore EL. Effectiveness of Multimodal Training on Functional Capacity in Frail Older People: A Meta-Analysis of Randomized Controlled Trials. J Aging Phys Act. 2018 Jul 1;26(3):407-418. doi: 10.1123/japa.2017-0188. Epub 2018 Jul 10 [ Links ]
7 Izquierdo M, Casas-Herrero A, Martinez-Velilla N, Alonso-Bouzon, C., Rodriguez-Manas, L., & en representación del Grupo de I. (2017). [An example of cooperation for implementing programs associated with the promotion of exercise in the frail elderly. European Erasmus + <<Vivifrail>> program]. Revista Española de Geriatria y Gerontologia, 52, 110-111. [ Links ]
8 Duaso E, Miralles R (dir), Tomás S (dir). Efecte d'un nou model d'atenció en pacients majors de 69 anys amb fractura de maluc ingressats a la unitat geriàtrica d'aguts (UGA) de l'Hospital d'Igualada [tesis doctoral en internet] [Barcelona]Universitat Autònoma Barcelona, 2015. Recuperado a partir de: https://ddd.uab.cat/pub/tesis/2016/hdl_10803_385728/edm1de1.pdf. [ Links ]
9 Gamboa-Arango A, Duaso E, Malafarina V, Formiga F, Marimon P, Sandiumenge M, Salgado MT, Escalante E, Lumbreras C, Tarrida A. Prognostic factors for dischrge to home residint at home 12 months afther hip fracture: an Anoia hip study. Aging Clin Exp Res. 2019 Aug 3. Doi: 10.1007/s40520-019-01273-0. [ Links ]
10 Gamboa-Arango A, Duaso E, Formiga F, Marimon P, Sandiumenge M, Salgado MT, , Escalante E, Lumbreras C, Tarrida APronostic factors of good functionality at 12 months of a hip fracture Malu. Anoia Study.. Rev Esp Cir Ortop Traumatol. 2019 Jul 31. Pi: S1888-4415(19)30110-9. Doi: 10.1016/j.recot.2019.06.007. [ Links ]
11 Gamboa-Arango A, Duaso E, Formiga F, Marimon P, Sandiumenge M, Salgado MT, , Escalante E, Lumbreras C, Tarrida APronostic factors of good functionality at 12 months of a hip fracture Malu. Anoia Study.. Rev Esp Cir Ortop Traumatol. 2019 Jul 31. Pi: S1888-4415(19)30110-9. Doi: 10.1016/j.recot.2019.06.007. [ Links ]
12 Duaso E, Casas A, Formiga F, Lázaro del Nogal M, Salvà A, Marcellán T y Navarro C, Grupo de Osteoporosis, Caídas y Fracturas de la Sociedad Española de Geriatría y Gerontología. Unidades de prevención de caídas y fracturas osteoporóticas. Propuesta del Grupo de Osteoporosis, Caídas y Fracturas de la Sociedad Española de Geriatría y Gerontología. Rev Esp Geriatr Gerontol. 2011;46(5):268-274. [ Links ]
13 Finnegan S., Bruce J., Skelton D., Withers E., Lamb S. Development and delivery of an exercise programme for falls prevention: the Prevention of Falls Injury Trial 8PreFIT). Physiotherapy 104(2018);72-79. [ Links ]
14 Bruce J., Lall R., Withers EJ., et al. A cluster randomised controlled trial of advice,exercise or multifactorial assessment to prevent falls and fractures in community-dwelling older adults: protocol for the prevention of falls injury trial (PreFIT). BMJ Open 2016;6:e009362. [ Links ]
15 Sherrington C, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019 Jan 31;1:CD012424. [ Links ]
16 Zhao R., Feng F., Wang X. Exercise interventions and prevention of fall-related fractures in older people: a meta-analysis of randomized controlled trials. Int J Epidemiol. 2017 Feb 1;46(1):149-161. doi: 10.1093/ije/dyw142. [ Links ]
17 Hopewell S., Copsey B., Nicolson P., Adedire B., Boniface G., Lamb S. Multifactorial interventions for preventing falls in older people living in the community: a systematic review and meta-analysis of 41 trials and almost 20 000 participants. Br J Sports Med. 2019 Aug 21. pii:bjsports-2019-100732. doi: 10.1136/bjsports-2019-100732. [ Links ]
18 Duaso E, Gamboa A, Marimón P, Sandiumenge M, Grados MD, Salgado MT, Casanovas MM, Garriga A. Mejorando la atencio´n del paciente mayor ingresado por fractura de cadera. ¿Hemos de avanzar?. Rev Esp Geriatr Gerontol. 2019;. [ Links ]
Received: December 08, 2021; Accepted: June 20, 2022
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
