










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkREC: Interventional Cardiology
versão On-line ISSN 2604-7276versão impressa ISSN 2604-7306
REC Interv Cardiol ES vol.5 no.2 Madrid Abr./Jun. 2023 Epub 18-Mar-2024
https://dx.doi.org/10.24875/recic.m22000336
IMAGES IN CARDIOLOGY
Atrial mass as a complication following complex percutaneous coronary intervention
aDepartamento de Cardiología, Hospital Universitario Fundación Jiménez Díaz, Madrid, España
bDepartamento de Radiología, Sección de Imagen Cardiaca, Hospital Universitario Fundación Jiménez Díaz, Madrid, España
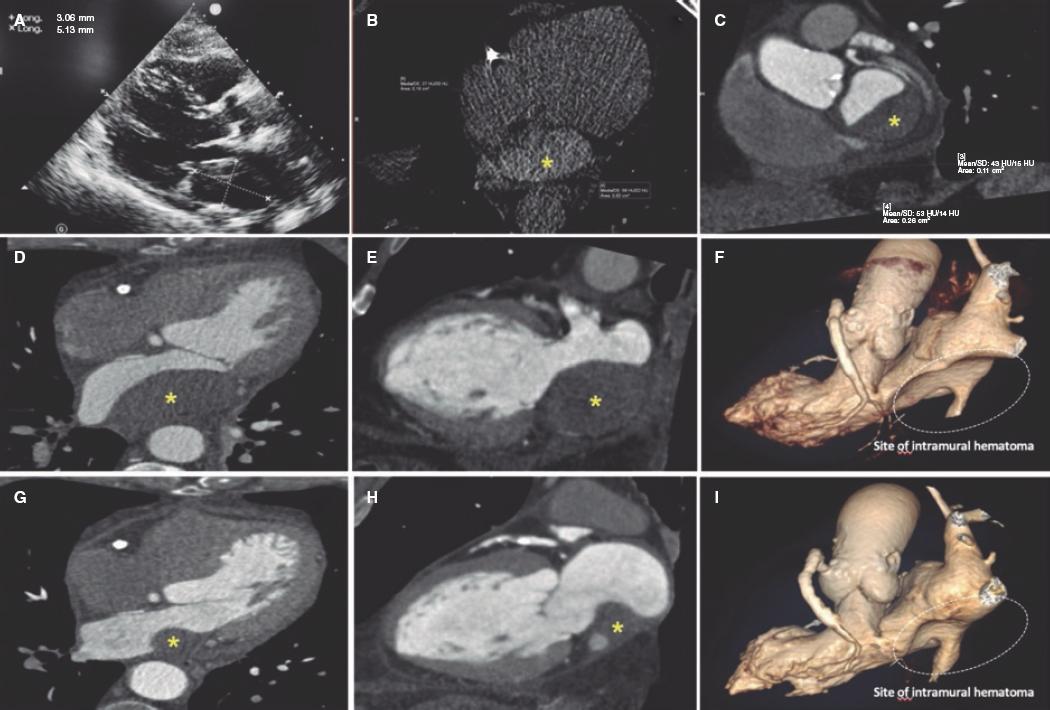
This is the case of a 75-year-old man who underwent coronary angiography due to new-onset dyspnea and left bundle branch block with a long, diffuse, and heavily calcified lesion with a maximum stenosis of 90% in his dominant right coronary artery. Patient was treated with complex percutaneous coronary intervention (PCI) (double-guidewire technique both hydrophilic wires guide catheter extension system, and compliant and non- compliant balloon dilatations), which eventually led to the successful distal-to-proximal implantation of 3 drug-eluting stents. A few hours later, he complained of pleuritic chest pain while remaining hemodynamically stable, and with a normal physical examination. Lab tests showed troponin I levels of 8 ng/mL (reference < 0.012 ng/mL). The echocardiogram showed no regional motion abnormalities, but revealed the presence of a 55.3 mm x 29 mm left atrial mass emerging from the posterior atrial wall almost occluding the complete atrial cavity without conditioning significant mitral valve dysfunction or an impaired transmitral flow. Pericardial effusion suggestive of hemopericardium was also described (figure 1A; video 1 of the supplementary data). Left atrial intramural hematoma (LAIH) was suspected and CCTA confirmed the lesion high attenuation (56 Hounsfield Units), which was suggestive of hematic component (*, figure 1B-F). The patient remained hospitalized until the stability of the lesion was confirmed (discharge size, 48 mm x 28 mm) while on dual antiplatelet therapy. After monthly clinical follow-ups, the control CCTA performed at 3 months confirmed significant reduction (30 mm x 20 mm) (*, figure 1G-I). LAIH is a rare complication associated with complex PCI procedures (probably caused while positioning the guidewires, penetrating distal vasculature, and causing the bleeding) being a potential cause for conduction disorders and hemodynamic instability. The patient's verbal consent was obtained.
AUTHORS' CONTRIBUTIONS
L. Nieto-Roca, M. Tomás-Mallebrera, and R. Carda Barrio: contributed substantially to the drafting of this case, obtained the patient's informed consent, and compiled all the images. They gave their approval to the manuscript final version. They take full responsibility for all aspects related to the article and commit themselves to investigating and solving all questions regarding the accuracy and truthfulness of any part of the work. J.A. Esteban-Chapel, and M.L. Martín-Mariscal contributed to the interpretation of the case, and the corresponding images. They gave their approval to the manuscript final version. They take full responsibility for all aspects related to the article and commit themselves to investigating and solving all questions regarding the accuracy and truthfulness of any part of the work.
Received: May 03, 2022; Accepted: July 05, 2022
 Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
