










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Eosinophils are inflammatory effector cells associated with various allergic and parasitic diseases [1]. They are characterized by the presence of large secondary granules containing four proteins: eosinophil cationic protein (ECP), eosinophil protein X (EPX), eosinophil peroxidase (EPO) and major basic protein (MBP), playing a role in the host's immune response to parasites and in the pathophysiology of chronic allergic responses. ECP (also known under the name ribonuclease 3 or Rnase3) is one of four proteins secreted by activated eosinophils and is currently the most widely used clinical marker of eosinophil activity in asthma and other inflammatory diseases [2]. Eosinophilic cells make up 1 to 4% of white blood cells circulating in the bloodstream. ECP is readily detectable in the blood with plasma levels of an average of 3 μg/L (serum 7 μg/L) in healthy subjects and correlates with the circulating number of eosinophils [3]. Human parasitic infections elicit an immune response associated with the production of cytokines by Th2 lymphocytes and eosinophilia. Eosinophilic infiltration into invaded tissues and skin is a common finding and therefore these cells are thought to play a specific role in the process of parasite destruction. Although still controversial, there is a theory that cytotoxic ECP deposition is part of the mechanism by which the immune system kills the parasite. In general, eosinophilia is also associated with an increase in circulating ECP levels [4, 5]. ECP has also been found around parasites in cutaneous and lymph nodes [6, 7]. The ability of ECP to kill or paralyze protozoa and helminths has been investigated in vitro and it has been found that high levels are required to respond to the parasite. Schistosoma mansoni larvae were incubated with 10 μM (190 μg/ml) ECP and 60% of them died. Concentrations of 50 μM (950 μg/ml) ECP killed 40% of Trypanosoma cruzi in about 6 hours and 90% of Brugia malayi in 48 hours [8, 9, 10].
Toxocariasis is a parasitic disease caused by the migration of nematode larvae of Toxocara spp. (mainly the canine and feline ascarids T. canis and T. cati) in the human body. Eosinophilia is one of the most common findings in Toxocarra spp. infection in both humans and animals [11]. Increased levels of blood eosinophils may be lacking in some patients [12]. Due to the variety of clinical symptoms and difficulty in determining the activity of the disease, the importance of various other markers is being explored to assist the main methods of diagnosing the disease (serology). A study by Magnaval et al. (2001) reported that ECP levels in patients with clinical and laboratory data of toxocariasis were significantly higher than in clinically healthy patients or those who were ill in the past, and according to the authors ECP may be a useful marker for distinguishing between present and past toxocariasis [13], especially in patients without eosinophilia. Another study found that in children with toxocariasis, the concentration of ECP was significantly higher than that of the control group and decreased significantly 6 months after therapy. According to the authors, ECP may be a marker of the activity of Toxocara spp. infection and determining its concentration may be useful for monitoring the effectiveness of administered therapy [14].
MATERIAL AND METHODS
STUDY DESIGN
It is a retrospective study of serum samples from individuals previously tested for toxocariasis. Samples were collected in the course of a diagnostic process in relation to clinical symptoms suggestive of toxocariasis and were taken in accordance with national law and good medical practice. After centrifugation for 15 min. at 1000 g samples were stored at -20° C until testing.
EXAMINED GROUPS
A group of sixty patients with clinical and serological data of toxocariasis (33 men and 27 women; ages 1 to 86 years; mean 37,2) were studied. The patients with leading symptom of eosinophilia were classified into 3 groups: mild eosinophilia (up to 10%), moderate eosinophilia (between 10-20%) and patients with high eosinophilia (over 20%).
The diagnosis of toxocariasis was confirmed by the presence of specific anti-Toxocara IgG antibodies in ELISA (RIDASCREEN® Toxocara IgG Rbiopharm) and the presence of specific bands in Western blot as confirmatory test (LD BIO). Twenty clinically healthy blood donors: 8 men and 12 women aged 35 to 49 (mean age 43) were used as control group.
DETERMINATION OF EOSINOPHIL CATIONIC PROTEIN (ECP) CONCENTRATION
ELISA (CUSABIO) commercial kit was used in this research. Detection range 1.56 ng/ml-100 ng/ml, sensitivity - 0.39 ng/ml. Standards (Standard) - S0-0 ng/ml (zero standard - sample diluent) and 2-fold dilution series - S1 - 1.56 ng/ml, S2 - 3.12 ng/ml, S3 - 6.25 ng/ml, S4 - 12.5 ng/ml, S5 - 25 ng/ml, S6 - 50 ng/ml, S7 - 100 ng/ml. Testing of serum samples was performed according to the manufacturer's instructions, and the ECP concentration was determined after photometric reading at 450 nm and construction of a Standard curve according to the used standards.
STATISTICAL WORK
Statistical data processing was performed with statistical package SPSS Version 20. The significance level at which the null hypothesis is rejected was p <0.05. The following methods of analysis were used: descriptive analysis (mean and standard deviation), parametric methods were used to look for statistical relationships between quantitative variables - ANOVA.
RESULTS
In patients with toxocariasis, the found ECP levels ranged from 1.56 ng/ml to 66.22 ng/ml (mean of 22.51 ng/ml ± 13.03 ng/ml standard deviation) for all studied patients. Levels of up to 16 ng/ml were found in 17 patients (28.3%); 31 (51.7%) were with levels from 16 to 30 ng/ml and 12 (20%) with levels above 30 ng/ml. ECP levels above the reference limit were found in 71.7% of patients with toxocariasis. Patients having ECP levels in the range of 16 to 30 ng/ml were with highest relative share.
In the control group of clinically healthy subjects, we found that the concentration of ECP ranged from 1.56 ng/ml to 18.84 ng/ml (mean 10.37 ng/ml ± 5.68 ng/ml standard deviation). Statistical data processing showed statistically significant differences in mean ESR levels between the two studied groups (ANOVA, p = 0.005).
No statistically significant differences in mean ECP values by gender were observed in the group of patients with toxocariasis (ANOVA, p = 0.682), although the mean ECP was slightly higher in male subjects - 23.14 ng/ml (min = 1.56 - max = 66.22 ng/ml) from the mean for women - 21.74 ng/ml (min = 6.62 - max = 46.86 ng/ml). Both sexes had the highest relative proportion of patients with ECP levels of 16 to 30 ng/ml - 42.4% of the males and 63% of the females. Among persons with an ECP concentration above 30 ng/ml (n = 12) predominated male patients (n = 9, 75%) (Table 1).
Table 1. Serum ECP levels in patients with toxicariasis by sex, age and clinical form of disease
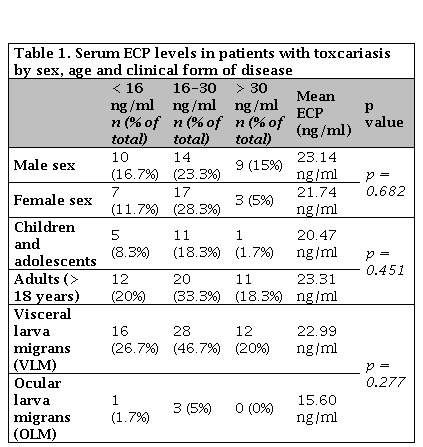
ECP: Eosinophil cationic protein.
Of the patients studied with toxocariasis, 17 were children and adolescents and 43 were adults (> 18 years). In both age groups, prevailed individuals with ECP values in range from 16 to 30 ng/ml (n = 11, 64.7% of children and n = 20, 46.5% of adults). No statistically significant differences (ANOVA, p = 0.451) were found between mean ECP concentrations in children (20.46 ng/ml ± 7.63 standard deviation) and in patients over 18 years of age (23.31 ng/ml ± 14.63 standard deviation). Most of the patients with values above 30 ng/ml were over 18 years of age (n = 11, 91.7%), and only one of the children was with an ECP concentration above 30 ng/ml (Table 1).
According to the clinical form of the disease, we found relatively higher levels of ECP among patients with visceral toxocariasis (mean 22.99 ng/ml ± 13.16 standard deviation) compared to those with ocular involvement (15.60 ng/ml ± 9.92 standard deviation), with these differences in values not being statistically significant (ANOVA,p = 0.277). Both clinical forms of the disease were dominated by patients with ECP levels between 16 and 30 ng/ml (50% of the patients with visceral form and 75% of the patients with ophthalmic disease). All patients with an ECP concentration above 30 ng/ml were with visceral toxocariasis (Table 1). Patients in whom we found ECP levels above 30 ng/ml (n = 12) were predominantly with clinically pronounced urticaria (n = 7, 58.3%) and pulmonary symptoms (pneumonia, chronic bronchitis) (n = 2, 16, 7%). Among patients with a leading clinical symptom of eosinophilia (n = 15), subjects with ECP levels from 16 to 30 ng/ml (n = 11, 73.3%) predominated, with only one person having ESR levels above 30 ng/ml. The mean concentration of ECP in eosinophilia patients was 21.52 ng/ml ± 7.72 standard deviation, which is value not significantly different from that in patients with other leading symptoms (Table 2) and there were no statistically significant differences (ANOVA, p = 0.371).
Table 2. ECO concentration (ng/ml) in patients with toxicariasis according to the leading clinical symptom
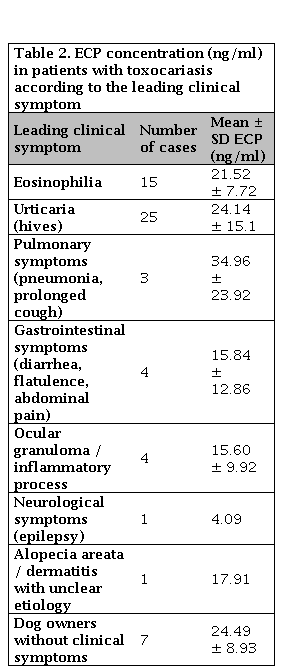
P value = 0.371. ECP: Eosinophil cationic protein; SD: Standard deviation.
To determine the correlation between the relative proportion of eosinophil cells in the peripheral blood and the concentration of ECP, the patients with leading symptom of eosinophilia were classified into 3 groups: mild eosinophilia (up to 10%), moderate eosinophilia (between 10-20%) and patients with high eosinophilia (over 20%). Although the established mean ECP levels in patients with high eosinophilia were higher (23.09 ng/ml ± 7.85 standard deviation), no statistically significant difference was found from patients with moderate (20.88 ng/ml ± 8.41 standard deviation) and mild (21.61 ng/ml; n = 1) eosinophilia (ANOVA, p = 0.904).
DISCUSSION
Eosinophils are pro-inflammatory cells that mediate allergic symptoms [15]. Their traditional role is related to the immune response in allergic diseases or parasitic infections [16]. They are involved in the development of the inflammatory reactions by secreting proteins and mediators of the inflammation [17]. At the site of inflammation, upon stimulation, eosinophils secrete toxic cationic proteins and this process is thought to be important for host defense [18], but the role of these proteins has not been fully understood yet. One of them is ECP (highly basic, cytotoxic, heparin binding ribonuclease), which is released by activated eosinophils [19]. Experimental data identify eosinophils and their granular proteins as significant participants in the inflammatory process in bronchial asthma [20] and in the interactions between parasite and host [21]. Secretion of the granular contents leads to damage of the bronchial epithelium and late asthmatic reactions, as well as to the killing and disintegration of larvae of various helminths [8, 10]. Since the discovery of ECP in 1977, a number of diagnostic kits have been developed to determine its level in biological fluids in various diseases. In infected individuals and those with hypereosinophilic syndrome, serum ECP may reach levels that are about 30 times increased compared to serum ECP levels in clinically healthy subjects [22].
The average ECP levels found by us in patients with toxocariasis exceed with statistically significant difference those in the control group of clinically healthy subjects and confirm existing data in the literature [13, 14]. The high relative share of patients with toxocariasis (about 72%) in which ECP values exceed the referent values gives us reason to believe that this protein is probably of key importance for the host defense against the parasite. We found no effect of age and gender on ECP production in patients with toxocariasis in this study. However, we found that in patients with visceral disease the mean serum concentrations of ECP were clearly higher than in those with ophthalmic disease, although the differences were not statistically significant. There are literature evidences for a correlation between serum ECP values and peripheral blood eosinophil counts [13, 23, 24], but no evidence has been found in patients whose leading symptom was eosinophilia. The lack of such correlation can be explained by the fact that serum granule proteins are derived not only from peripheral cells but also from activated eosinophils in the tissues. Eosinophils are actively involved in the tissue-dwelling inflammatory reaction and the circulating pool of eosinophils represents a small fraction of total eosinophil mass and lack of blood eosinophilia does not mean lack of eosinophilia in the body [25]. Eosinophilia in peripheral blood is an indicator of increased eosinophil migration. Leaving the bone marrow, the eosinophils remain in circulation for 8-12 hours, and then migrate to the tissues, where they remain for up to 10 days. The number of eosinophils in tissues is 200-300 times higher. The level of ECP reflects the activation and degranulation of eosinophils in target organs. Therefore, in monitoring eosinophil activity, the determination of ECP may be is a more reliable indicator. Eosinophilia is a characteristic laboratory finding in toxocariasis, but it has different kinetics in individual patients. Eosinophilia in peripheral blood is proportional to the tissue eosinophilia, where a local reaction to the Toxocara larvae or their antigens remaining in the tissues after larval migration develops [26]. The occurrence of eosinophilia in patients with toxocariasis is evidence for activity of the infection and for presence of antibody response. Increases in ECP levels have been identified not only in patients with a leading symptom of eosinophilia, which leads us to believe that an ECP concentration determination in patients with toxocariasis may be useful in establishing the disease activity.
Undoubtedly, the clinical interpretation of established levels of serum ECP is difficult as the protein is involved in a large number of biological reactions, characterizing it as a non-specific marker. However, determining its levels in patients with toxocariasis may provide an additional information, that when is analyzed together with serologic data, can improve the diagnosis of the disease. Our study may give us reason to believe that serum levels of ECP could serve as an additional marker indicating recent infection, especially in patients without marked increase in the blood eosinophils and further studies of larger number of patients should be conducted to confirm the finding.

